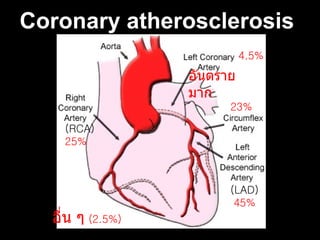
Risk factors Olderage ( M > 40 , F > 50 ) Male 3 -5 times > Female Tobacco smoking Hypercholesterolemia ( especially high LDL and low HDL) DM HT Obesity (BMI > 30 kg/m²) Low Physical activity Stress genetic predisposition Hyperhomocysteinemia (high homocysteine, a toxic blood amino acid that is elevated when intakes of vitamins B2, B6, B12 and folic acid are insufficient)
7.
Symptom Chest pain:a sensation of tightness, pressure, or squeezing. pain zones (dark red = most typical area, light red = other possible areas)
Symptom Jaw pain, toothache, headache Shortness of breath Nausea, vomiting, and / or general epigastric discomfort Sweating Heartburn and/or indigestion Arm pain (more commonly the left arm, but may be either arm) Upper back pain General malaise (vague feeling of illness) No symptoms (Approximately one quarter of all heart attacks are silent, without chest pain or new symptoms. Silent heart attacks are especially common among patients with DM .)
10.
Physical examination Maybe comfortable, or restless and in severe distress Increased respiratory rate. A cool and pale skin Some patients have low-grade fever (38–39 °C). BP may be elevated or decreased, Pulse irregular
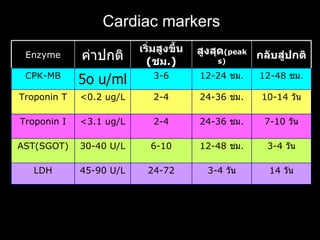
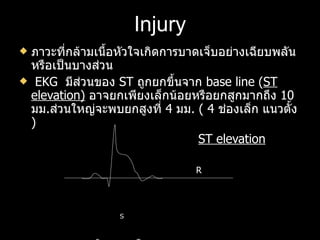
Diagnostic criteria WHOcriteria two (probable) or three (definite) of the following criteria are satisfied: Clinical history of ischaemic type chest pain lasting for more than 20 minutes Changes in serial ECG tracings Rise and fall of serum cardiac biomarkers such as ck-MB and troponin OR troponin rise + either typical symptoms, pathological Q waves, ST elevation or depression or coronary intervention are diagnostic of MI. *Note : Troponin T increases within 3-12 hours from the onset of chest pain, peaks at 24-48 hours, and returns to a normal level over 5-14 days
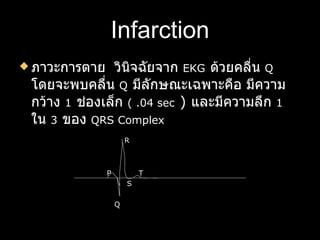
Infarction ภาวะการตาย วินิจฉัยจาก EKG ด้วยคลื่น Q โดยจะพบคลื่น Q มีลักษณะเฉพาะคือ มีความกว้าง 1 ช่องเล็ก ( .04 sec ) และมีความลึก 1 ใน 3 ของ QRS Complex R P T S Q
20.
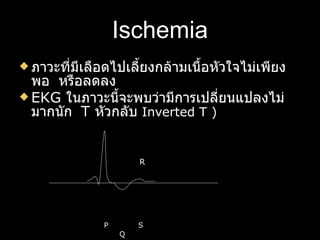
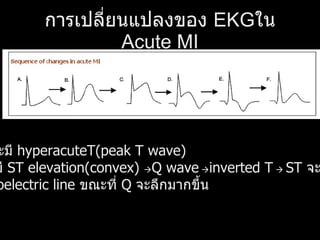
การเปลี่ยนแปลงของ EKGใน Acute MI เริ่มแรกจะมี hyperacuteT(peak T wave) ต่อมาจะมี ST elevation(convex) Q wave inverted T ST จะเริ่มลดลง กลับสู่ isoelectric line ขณะที่ Q จะลึกมากขึ้น
21.
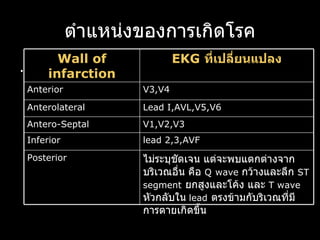
ตำแหน่งของการเกิดโรค . ไม่ระบุชัดเจนแต่จะพบแตกต่างจากบริเวณอื่น คือ Q wave กว้างและลึก ST segment ยกสูงและโค้ง และ T wave หัวกลับใน lead ตรงข้ามกับริเวณที่มีการตายเกิดขึ้น Posterior lead 2,3,AVF Inferior V1,V2,V3 Antero-Septal Lead I,AVL,V5,V6 Anterolateral V3,V4 Anterior EKG ที่เปลี่ยนแปลง Wall of infarction
22.
Indications for admit E valuating chest pain Recurrent Chest Pain Ischemic ECG Changes Ventricular Arrythma Positive Stress Test Positive Imaging Positive Echo Cardiac enzymes Positive
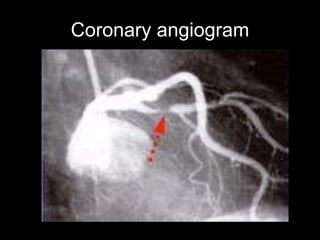
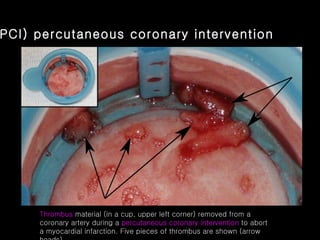
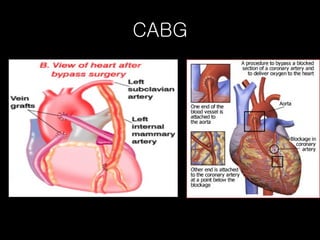
(PCI) percutaneous coronary intervention Thrombus material (in a cup, upper left corner) removed from a coronary artery during a percutaneous coronary intervention to abort a myocardial infarction. Five pieces of thrombus are shown (arrow heads)
Prevention of CAD Don't smoke. Control your blood pressure Check your cholesterol Exercise regularly. Maintain a healthy weight. Eat a heart-healthy diet. Get regular medical checkups Manage stress.