Downloaded 13 times
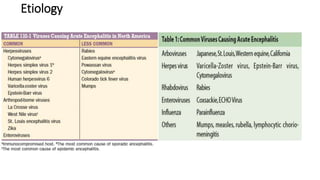
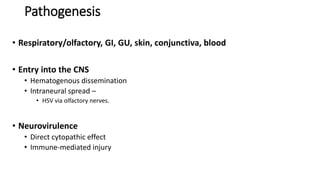
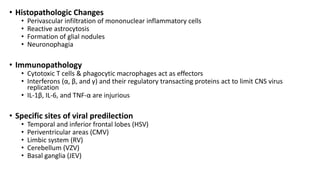
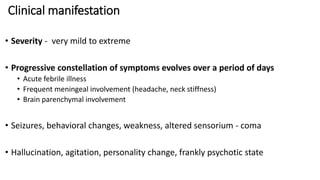

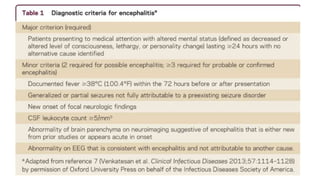



This document provides information on acute encephalitis syndrome, including its definition, epidemiology, etiology, pathogenesis, clinical manifestations, laboratory diagnosis, differential diagnosis, and management. Acute encephalitis syndrome is defined as an acute onset fever with changes in mental status or seizures. It is commonly caused by viruses and can involve inflammation of the brain tissue. Diagnosis involves examination of CSF and imaging studies. Treatment focuses on supportive care and antiviral medications like acyclovir.













































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)









