The inflammationof the brain substance may be
caused by viruses- bacteria- fungi-drugs –post
infectious and radiation.
This is mostly due to herpes simplex virus
followed by Japanese encephalitis.
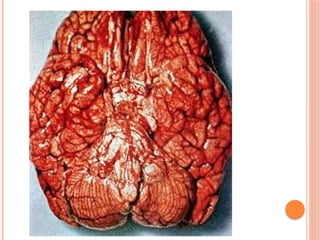
The liable part of the brain are the temporal
lobes.
4.
Clinical features:
It affects young adults usually. The clinical suspicion
will be directed by a careful history to indentify the
sequence of:
Fever
Headache
Confusion
convulsions
5.
It isimportant to enquire about behavioral
changes that are easily observed by the family
members or friends.
Travelling history (epidemics) is important as
well as recent vaccination co morbid conditions
like DM.
6.
The mainfeatures in the acute phase may be
only a toxic febrile patient who has confusion
(low GCS). Focal signs may appear i.e. cranial
neuropathy or papilloedema.
Detailed medical examination is essential
including the general and all systems.
Temperature charts and other vitals.
The planof investigations must include:
Brain MRI
LP and CSF analysis
9.
Other diseasesthat that may present like this
includes:
Vascular events : Stroke- SDH- AVM
SOL: Tumors- Granulmoa-Abscesses
Chronic infections: TB Meningitis
Chronic inflammation: Sarcoidosis- SLE
10.
All thesediseases as well as viral encephalitis
may show focal signs or cranial nerve’s palsy at
presentation.
Viral encephalitis may end with weakness,
dystonia or cognitive disability.
11.
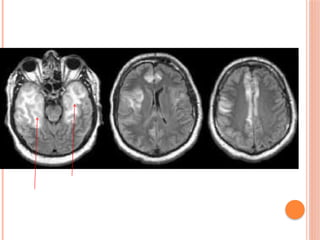
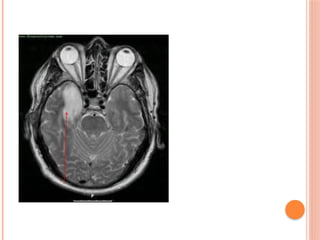
MRI Brainis abnormal specially at day 3
onwards.
Bilateral or unilateral temporal signals are
characteristic. Other areas may be affected in
other viruses or medical diseases.
14.
THIS IS ANESSENTIAL TEST
FOR THE DIAGNOSIS
CSF analysis:
Clear fluid
May be under tension
High number of lymphocytes over 5 cells-1000 mainly
lymphocytes. May be normal count or neutrophils early in
the course.
Raised proteins 0.5-1g/dl
Glucose may be normal / mild reduction.
Negative Gram stain ZN stain and culture.
PCR for HSV 95% sensitivity and specificity.
15.
Management:
Thesepatients are in great need of
vital signs assessment and
management.
They are liable to arrhythmias, breathing
abnormalities up to respiratory failure, central
temperature issues and fluctuation of BP.
They are usually managed in the ICU with full
support in the case of low GCS. This includes
mechanical ventilation as elective or emergency.
16.
The lowGCS and seizures much compromise
their breathing and the hypoxia will worsen the
cerebral damage hence worsening the outcome.
Antibiotics must be introduced for documented
infections.
17.
BAD OUTCOME ISASSOCIATED
WITH 2 DAYS OR MORE DELAY
IN TREATMENT
Time is brain
Time is memory
Time is knowledge
Time is concept
Time is vision
Time is hearing
18.
UNTREATED HSV ENCEPHALITIS
MORTALITYIS 40-70%
SURVIVORS MAY HAVE LONG TERM
DISABILITY.
The drug of choice is aciclovir infusion as
10mg/kg 8 hourly infused in normal saline over
40-0 minutes.
Duration of treatment is 2-3 weeks.
Dose must be adjusted in renal impairment.
Antiepileptic drugs are usually needed in these
patients in the form of phenytoin infusion 100mg
8 hourly plus oral carbamazepine or lamotigene
or valproate.
19.
Antipyretics areessential.
Cold sponging and low room temperature.
Well balanced nutrition and hydration to face the
high metabolic needs.
20.
OTHER LESS COMMONTYPES
ADEM: Acute disseminated encephalomyelitis
is a disease of children and adolescents. It shows
similar lesions on MRI to multiple sclerosis but is
monphasic condition and lesions are larger than
MS plaques.
HEMORRHAGIC POST INFECTIOUSENCEPHALITIS HURT’S DISEASE:
A very serious type of encephalitis that is post
infectious with extensive brain substance
bleeding. Mortality rate reaches 85%.
23.
NMDA RECEPTOR ENCEPHALITIS
A rare disease of young females. It is related to
the presence of ovarian teratoma that secrets
antibodies. Only removal of the tumor is
associated with remission of the condition.