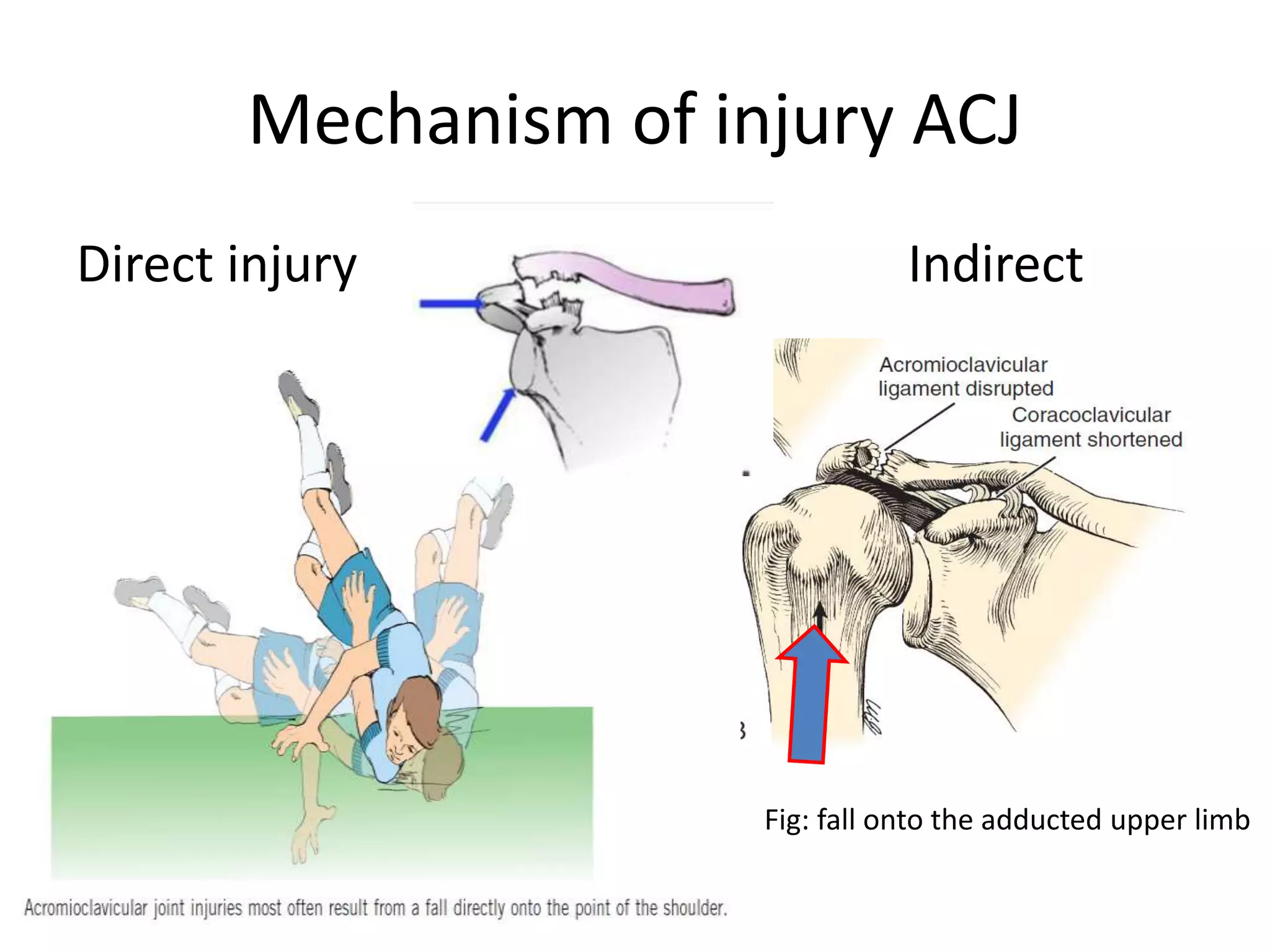
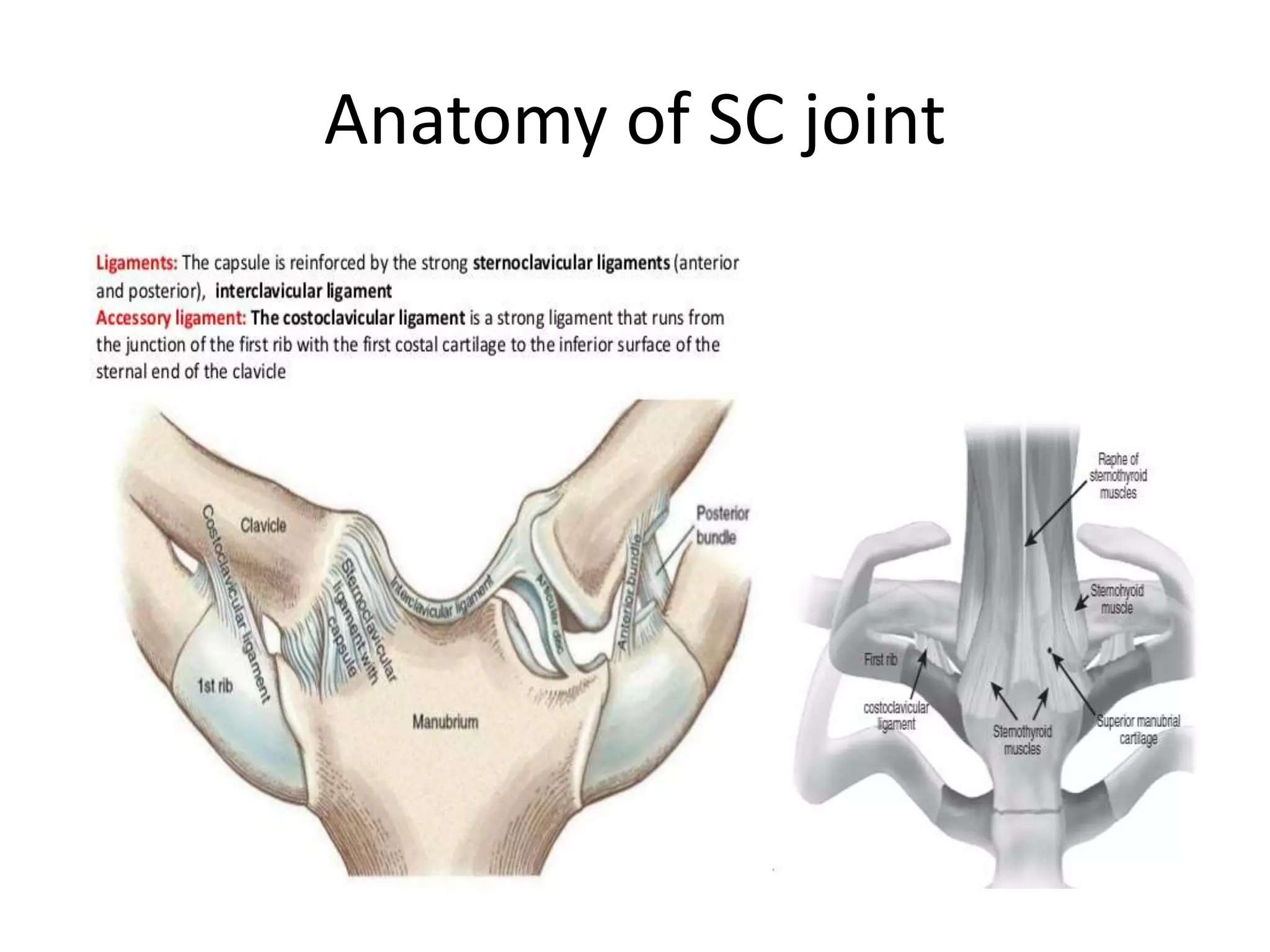
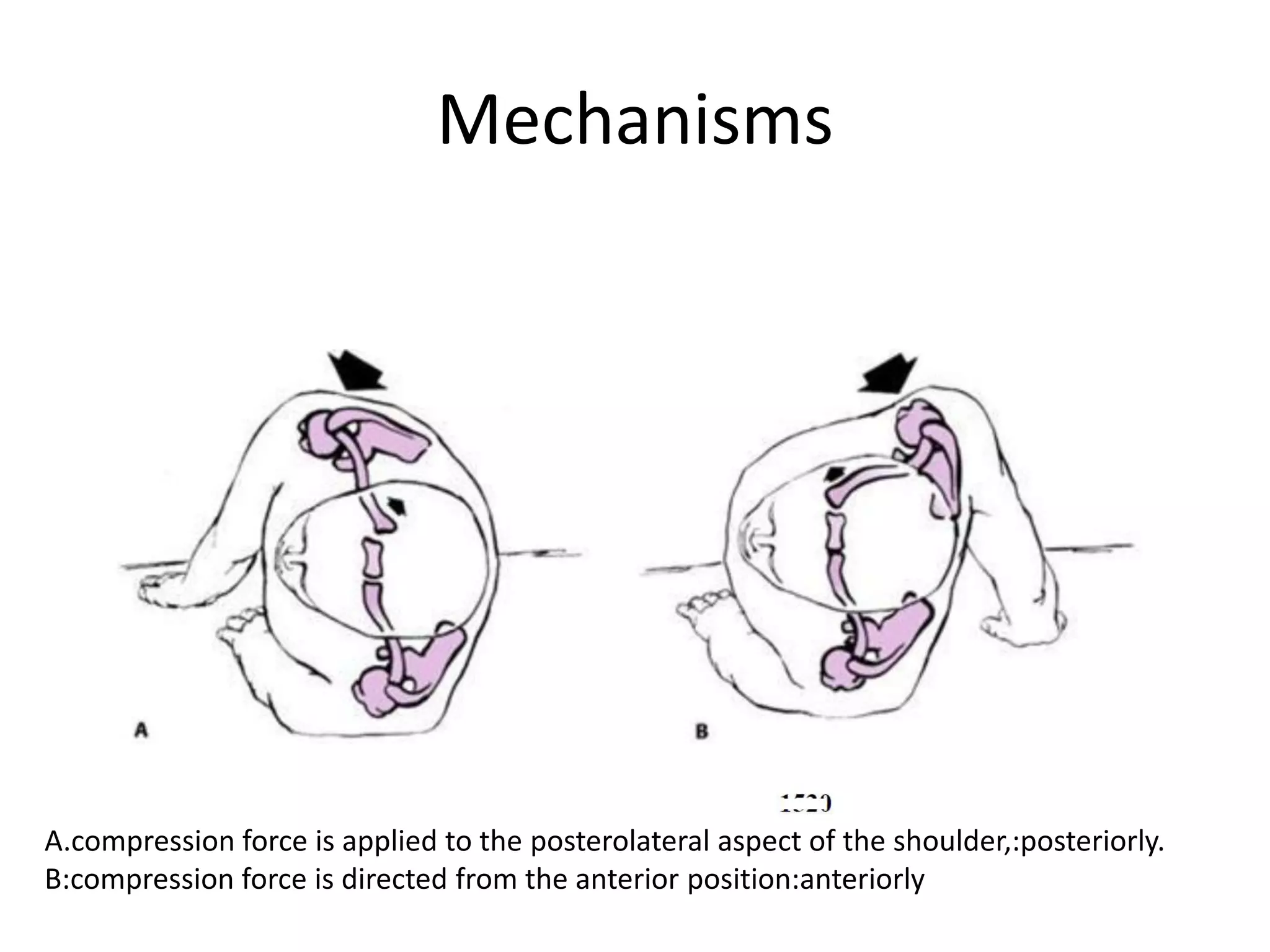
1) Acromioclavicular (AC) and sternoclavicular (SC) joint injuries are caused by direct or indirect trauma and can range from minor sprains to severe dislocations.
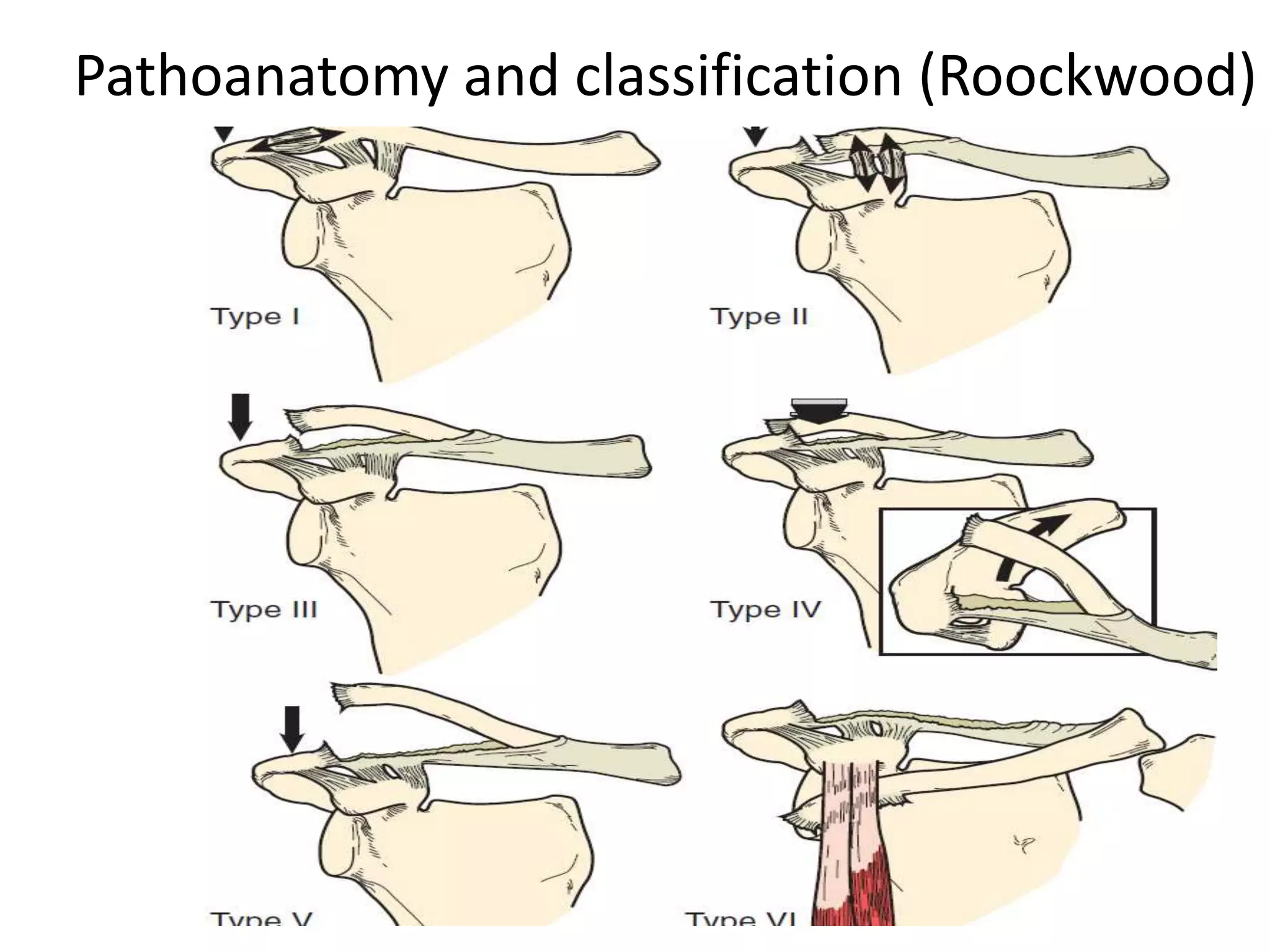
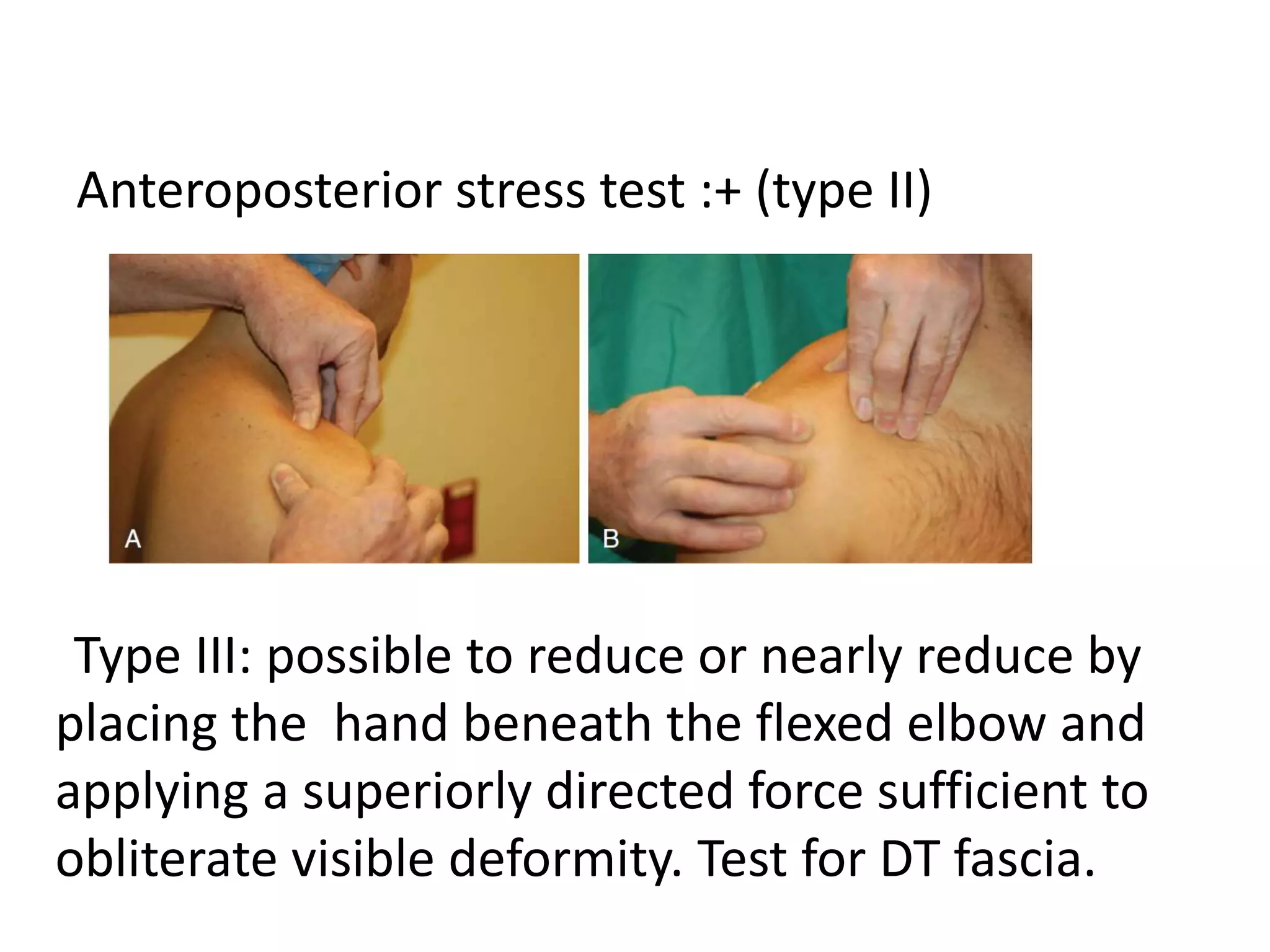
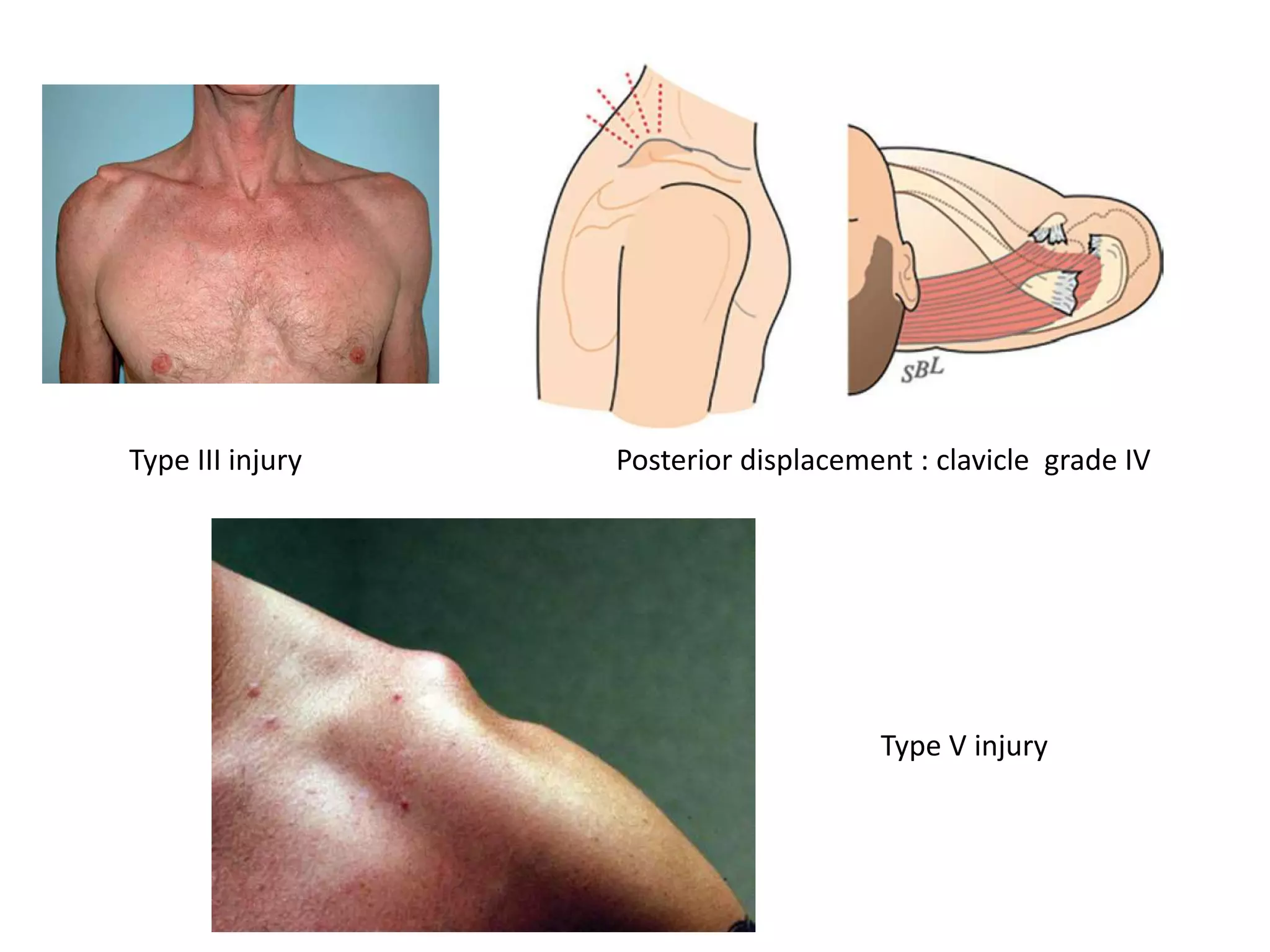
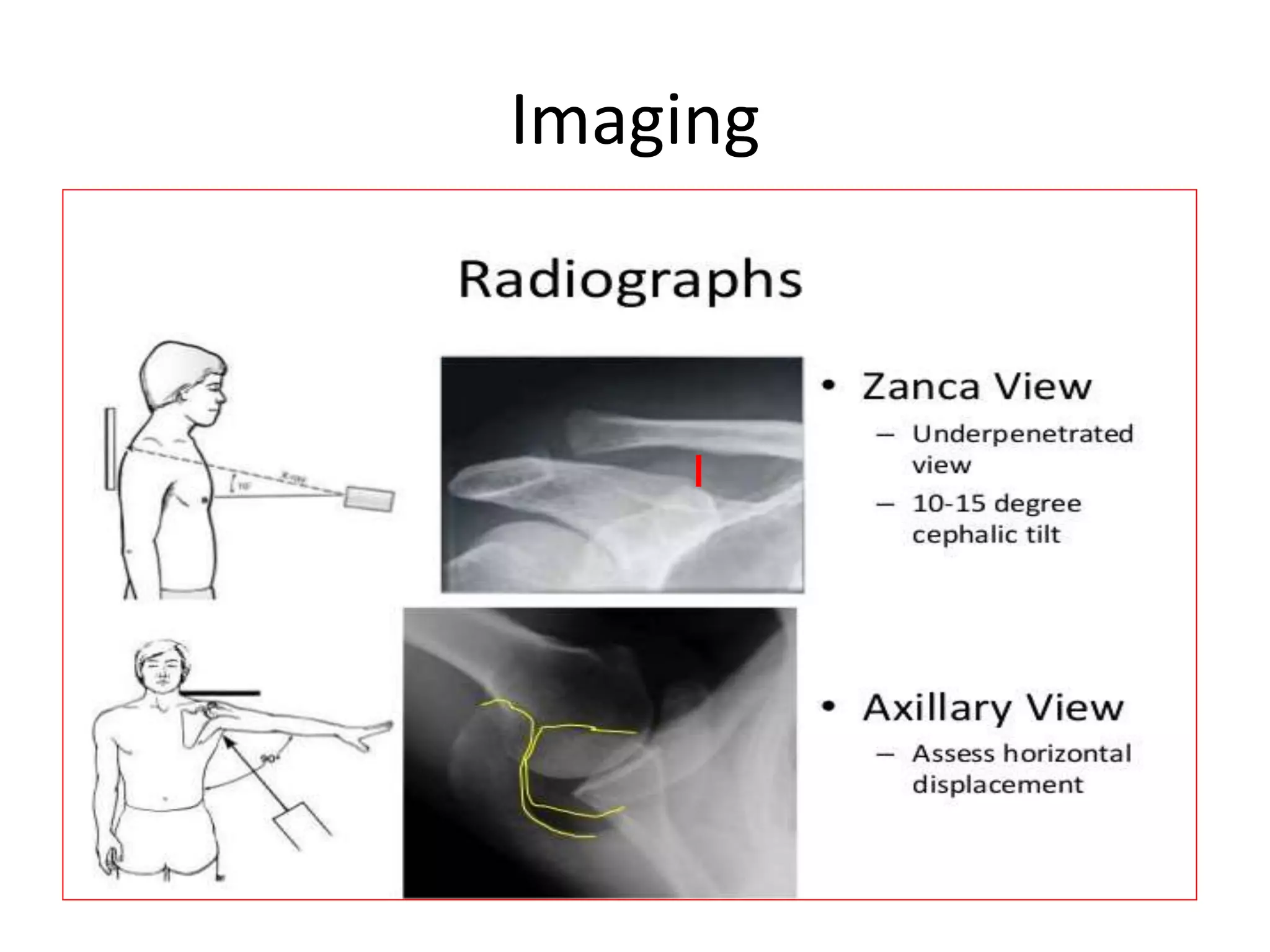
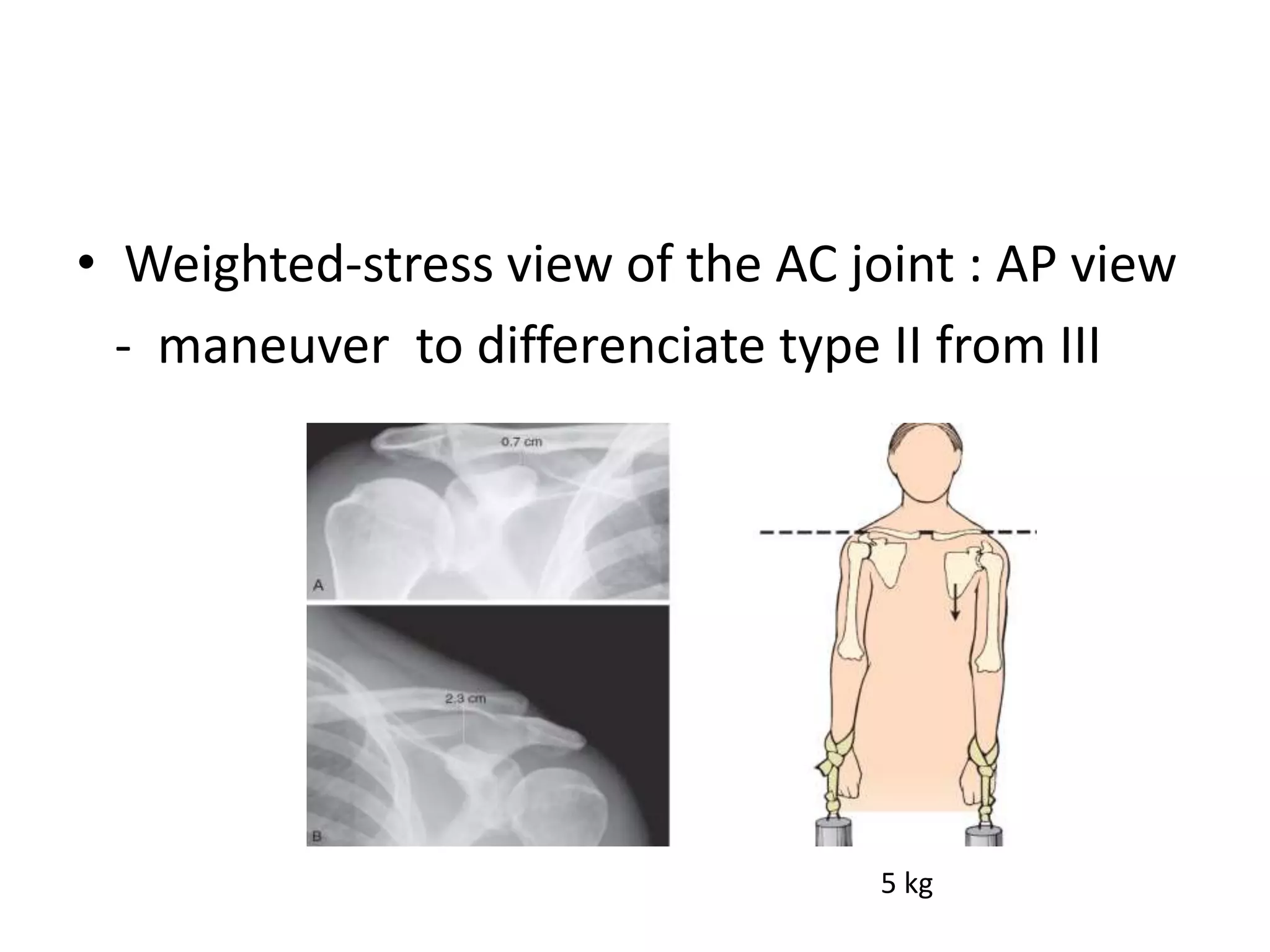
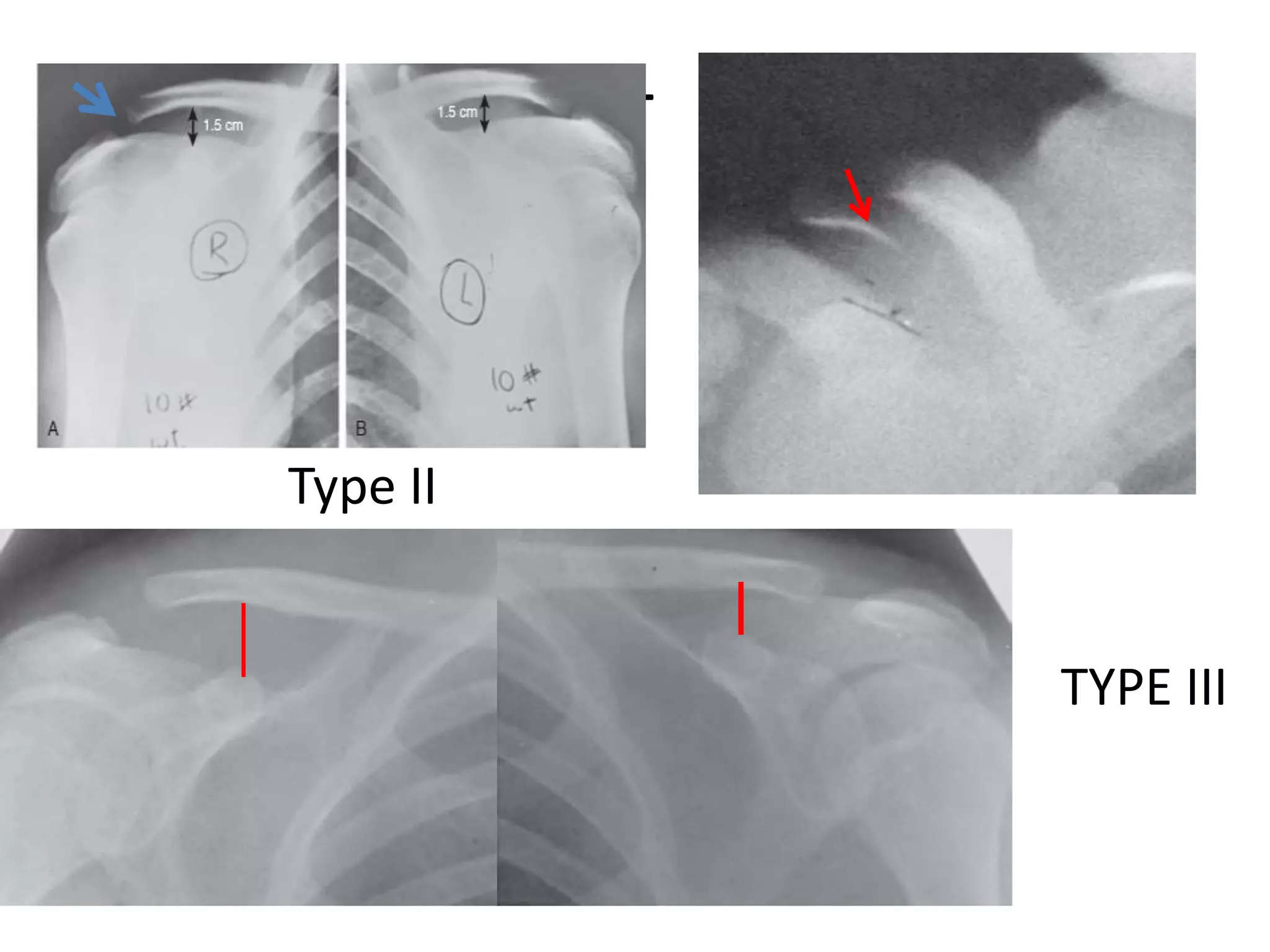
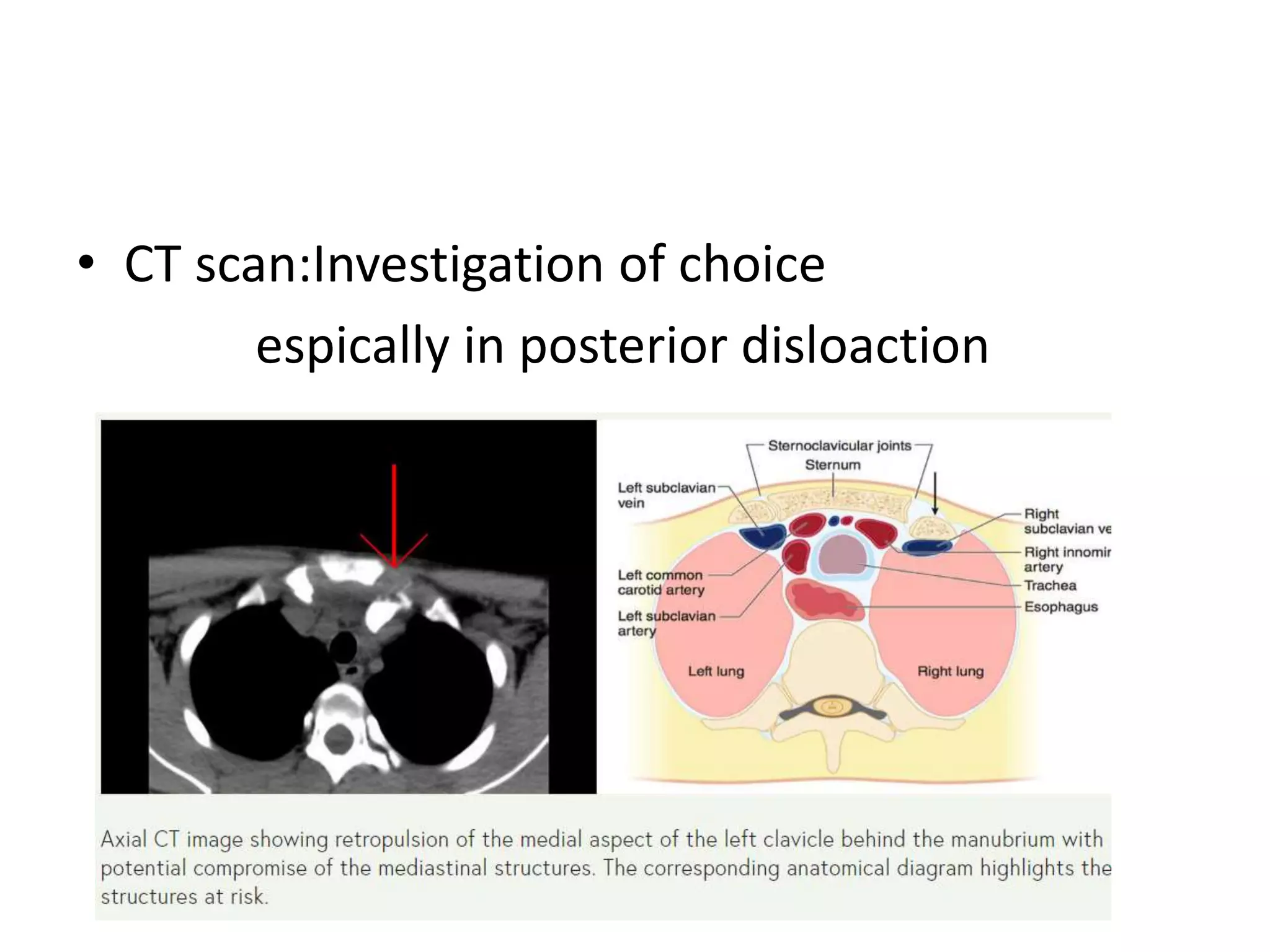
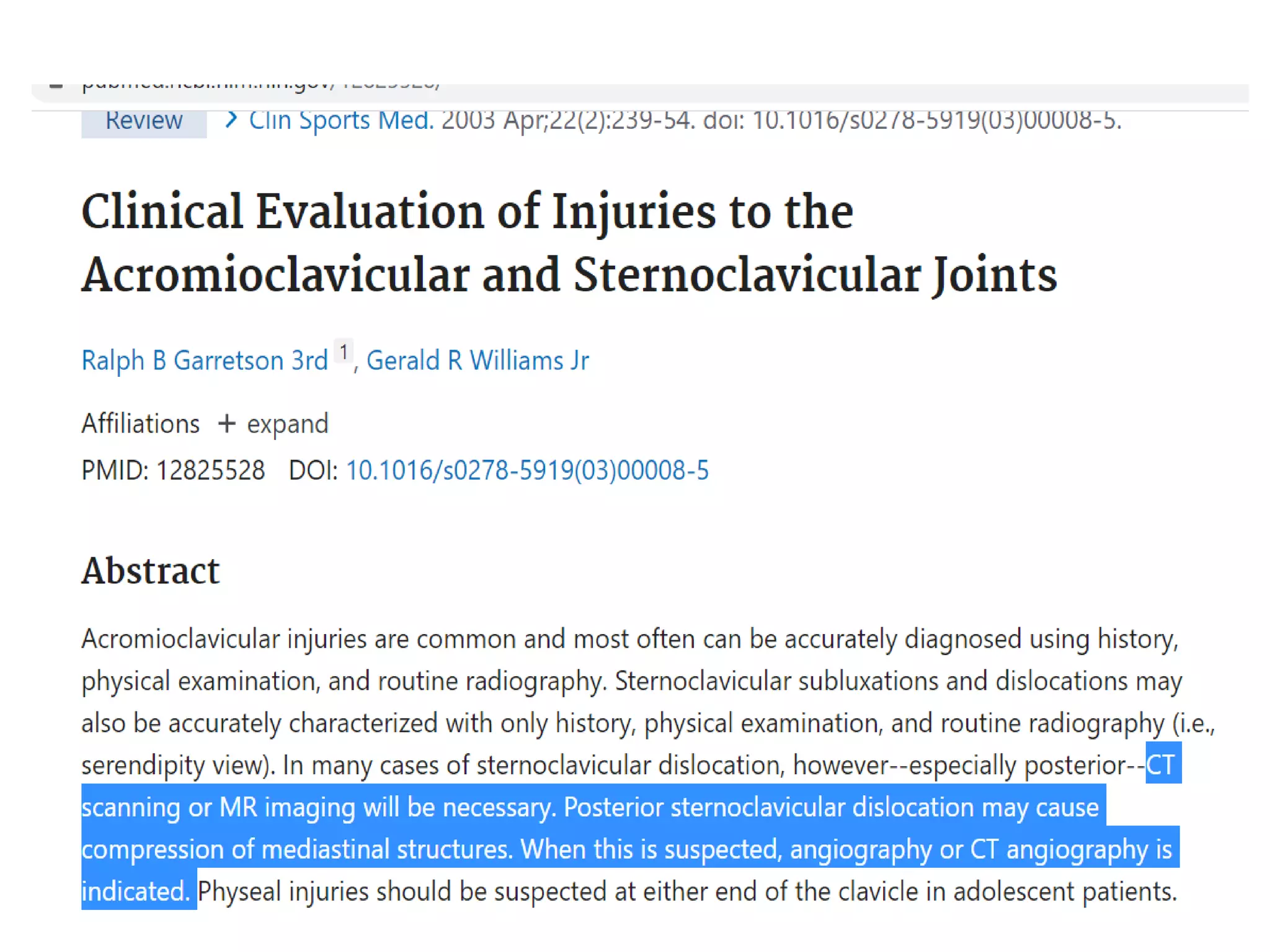
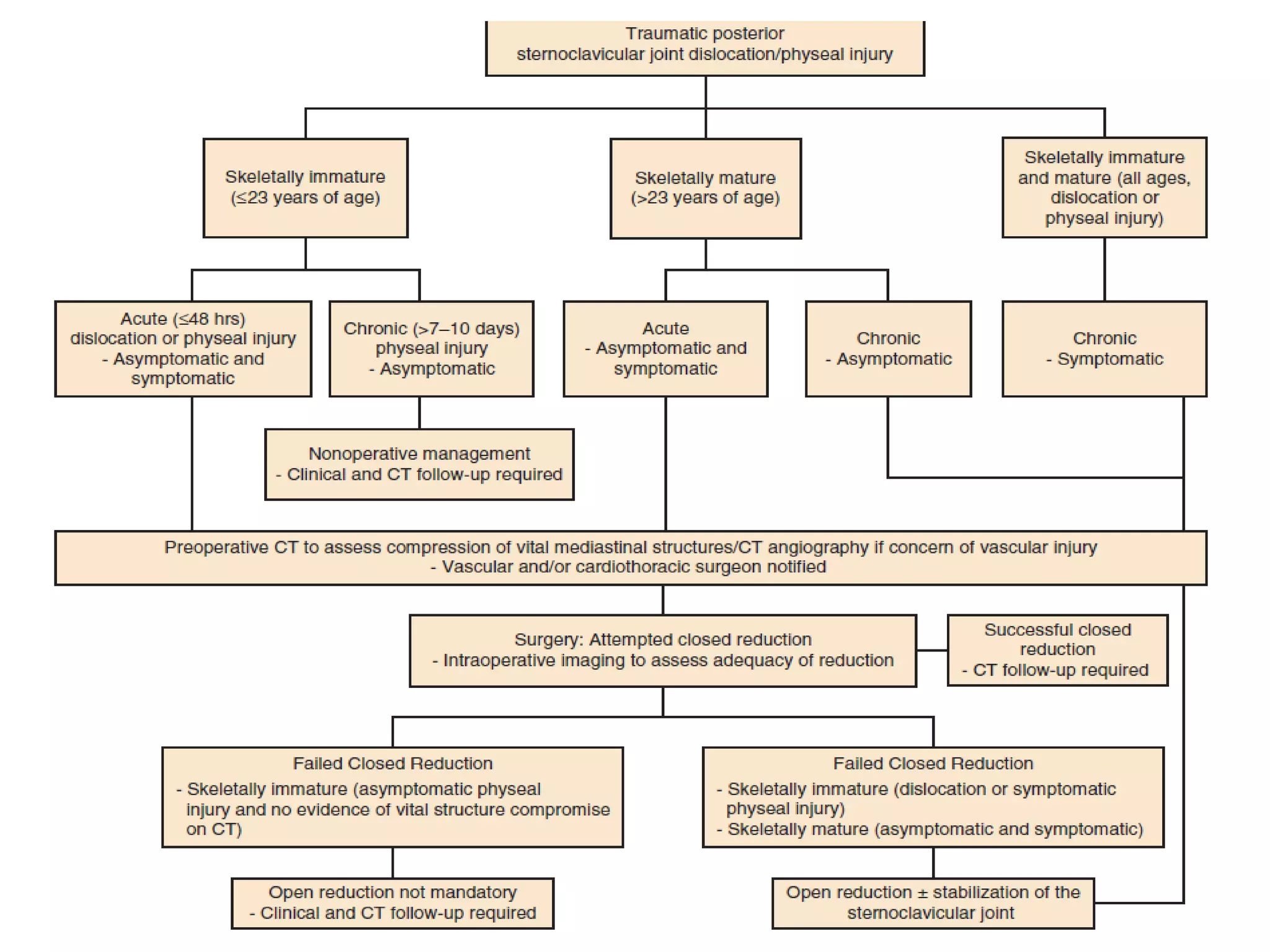
2) Imaging such as X-rays and CT scans are used to classify AC injuries using the Rockwood classification and assess severity of SC injuries.
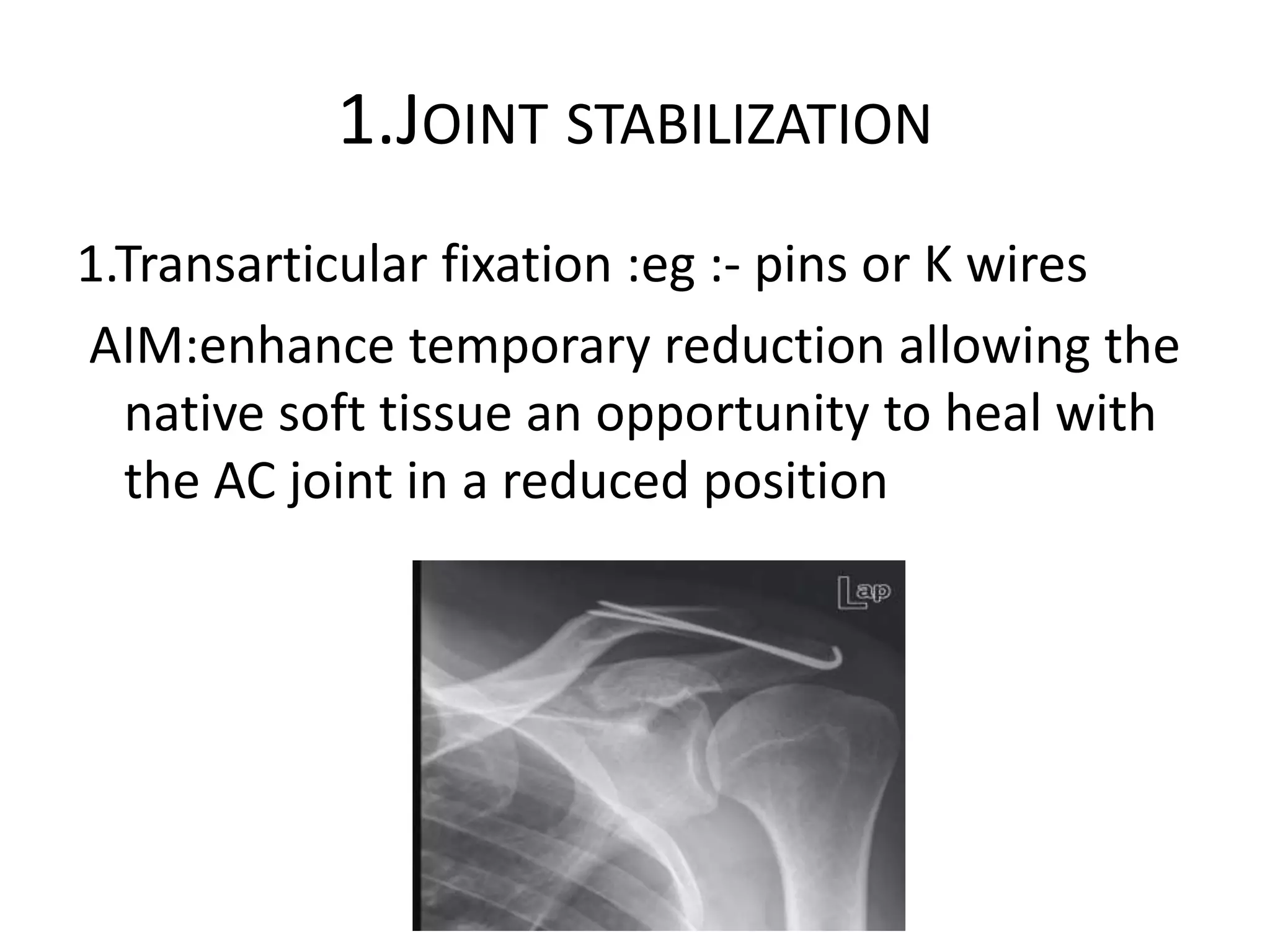
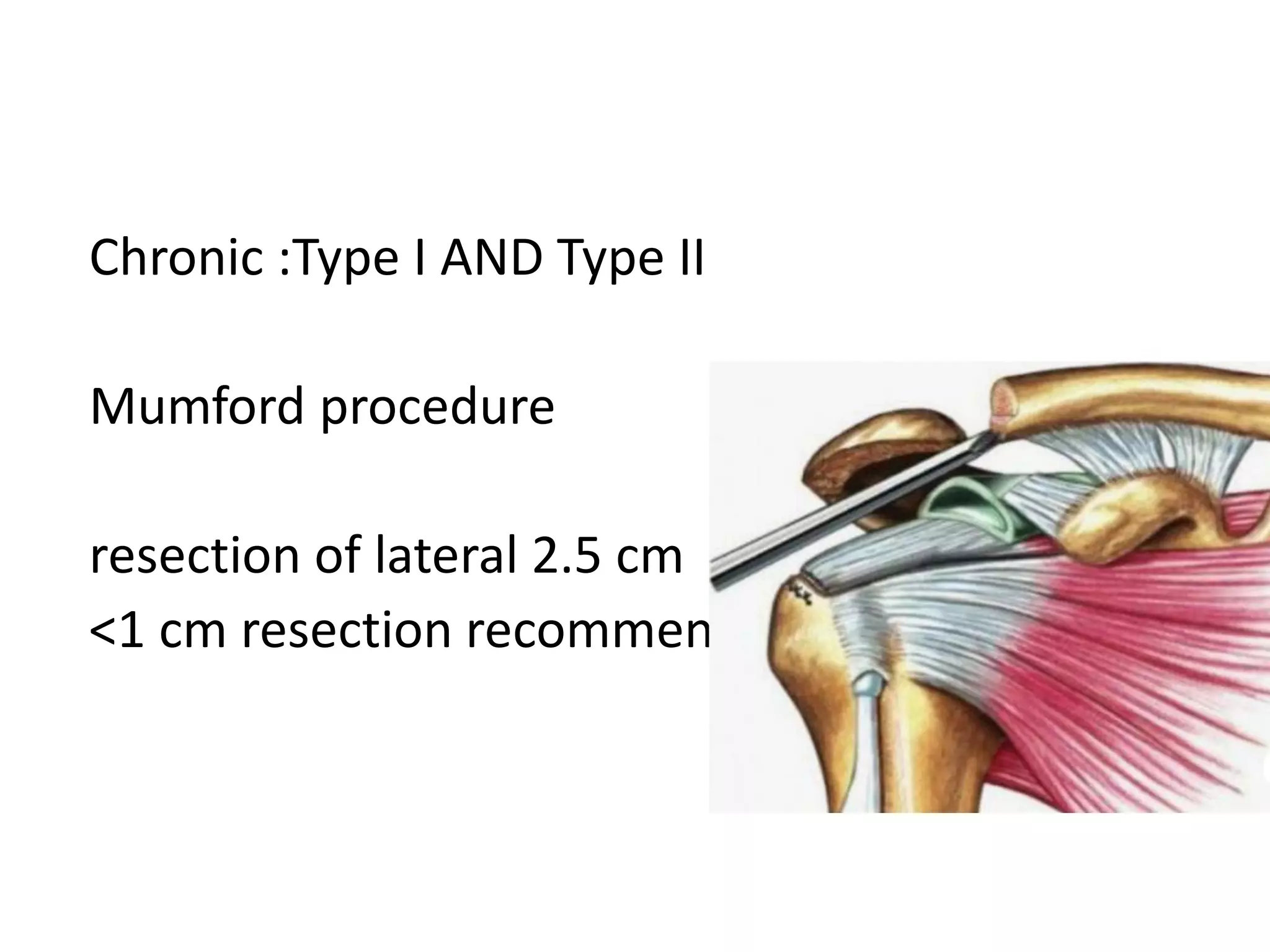
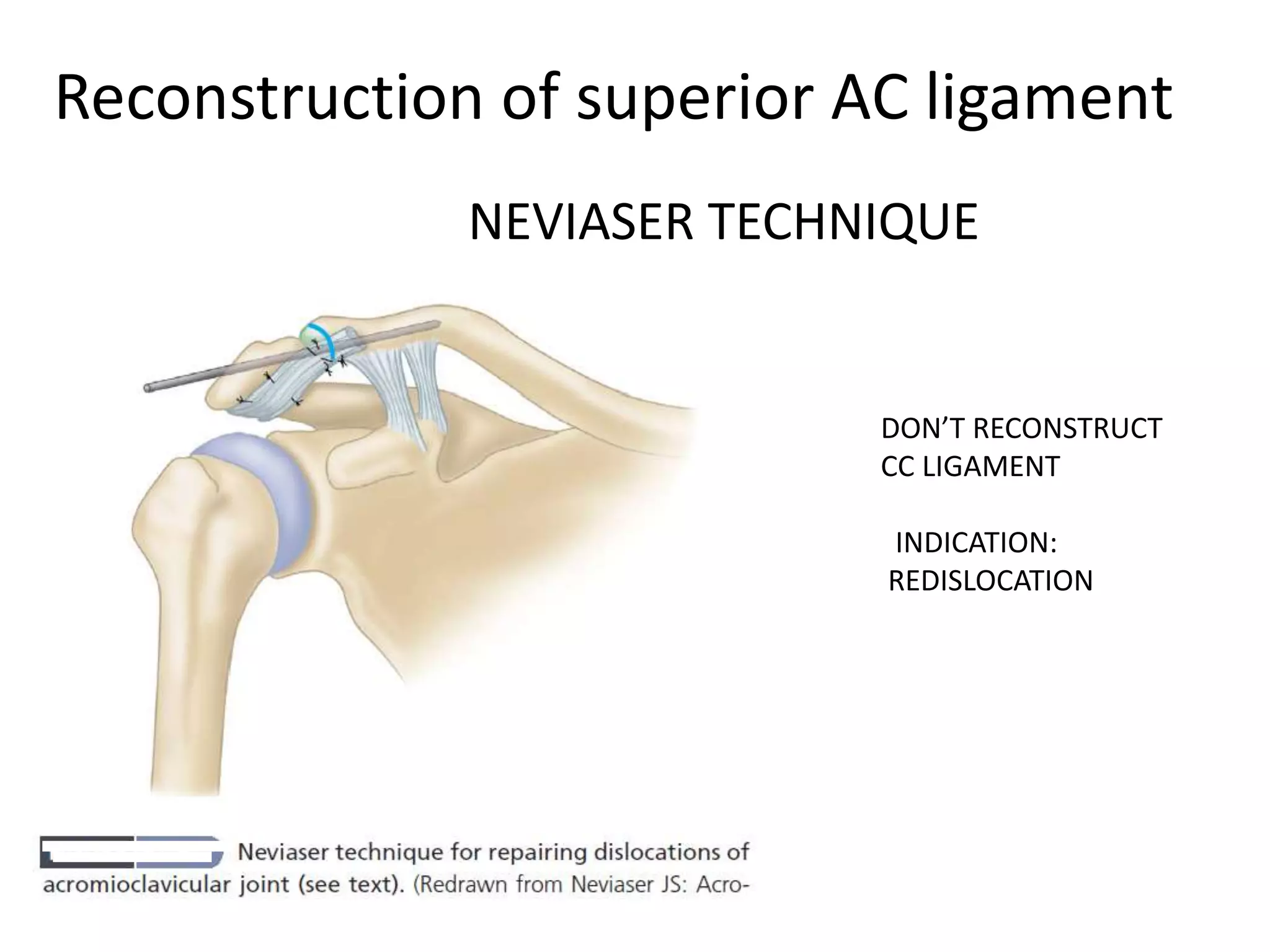
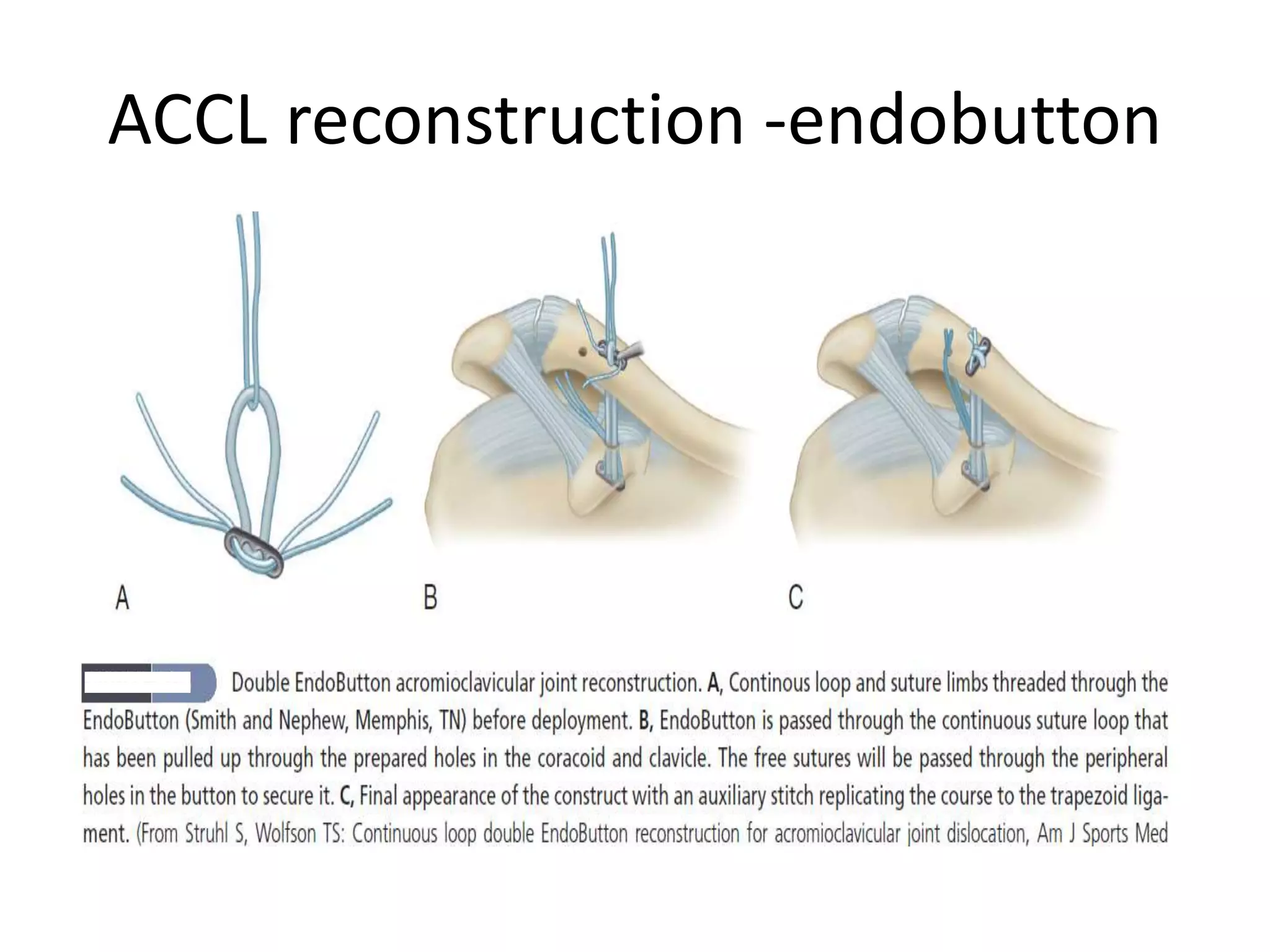
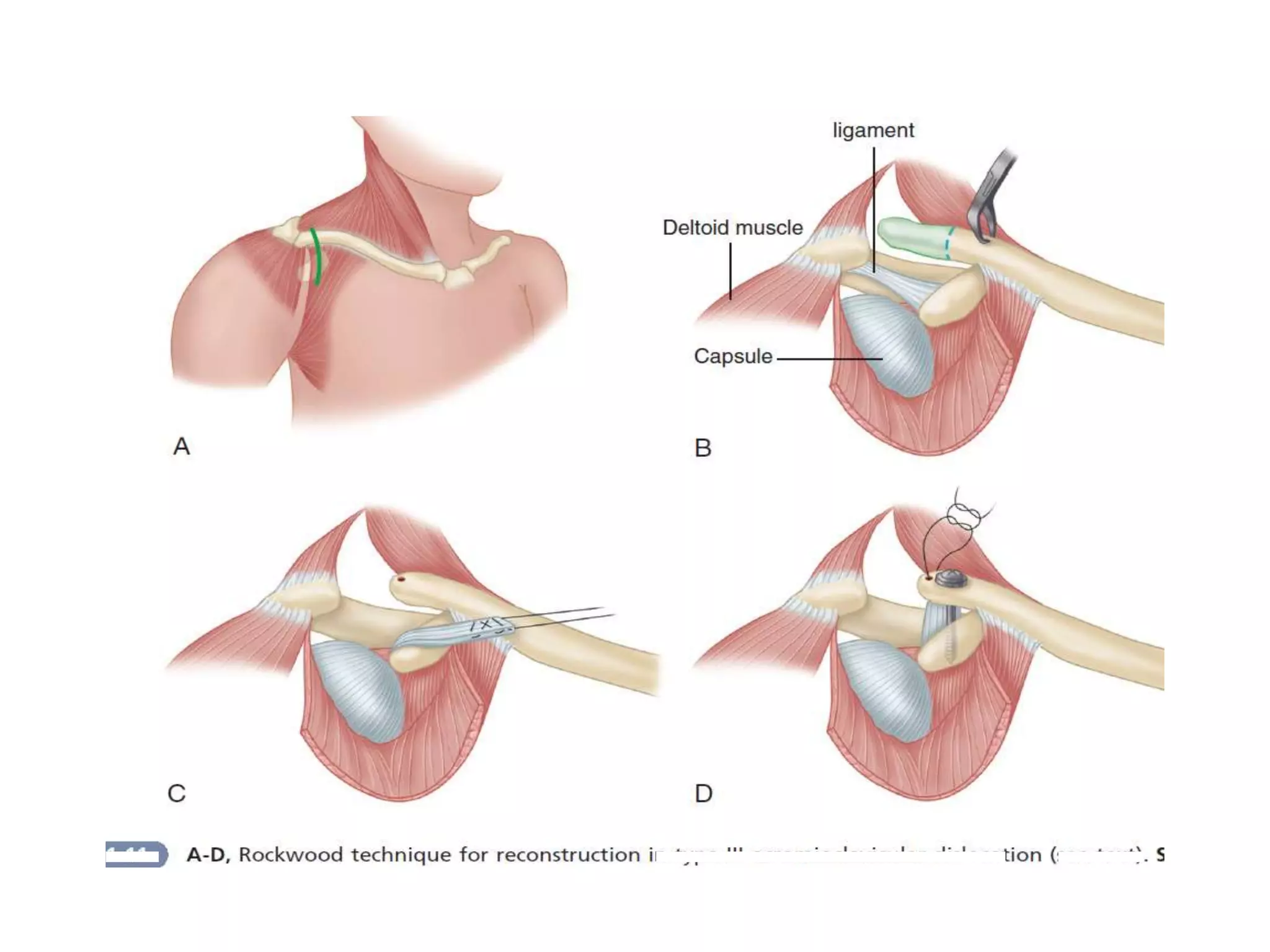
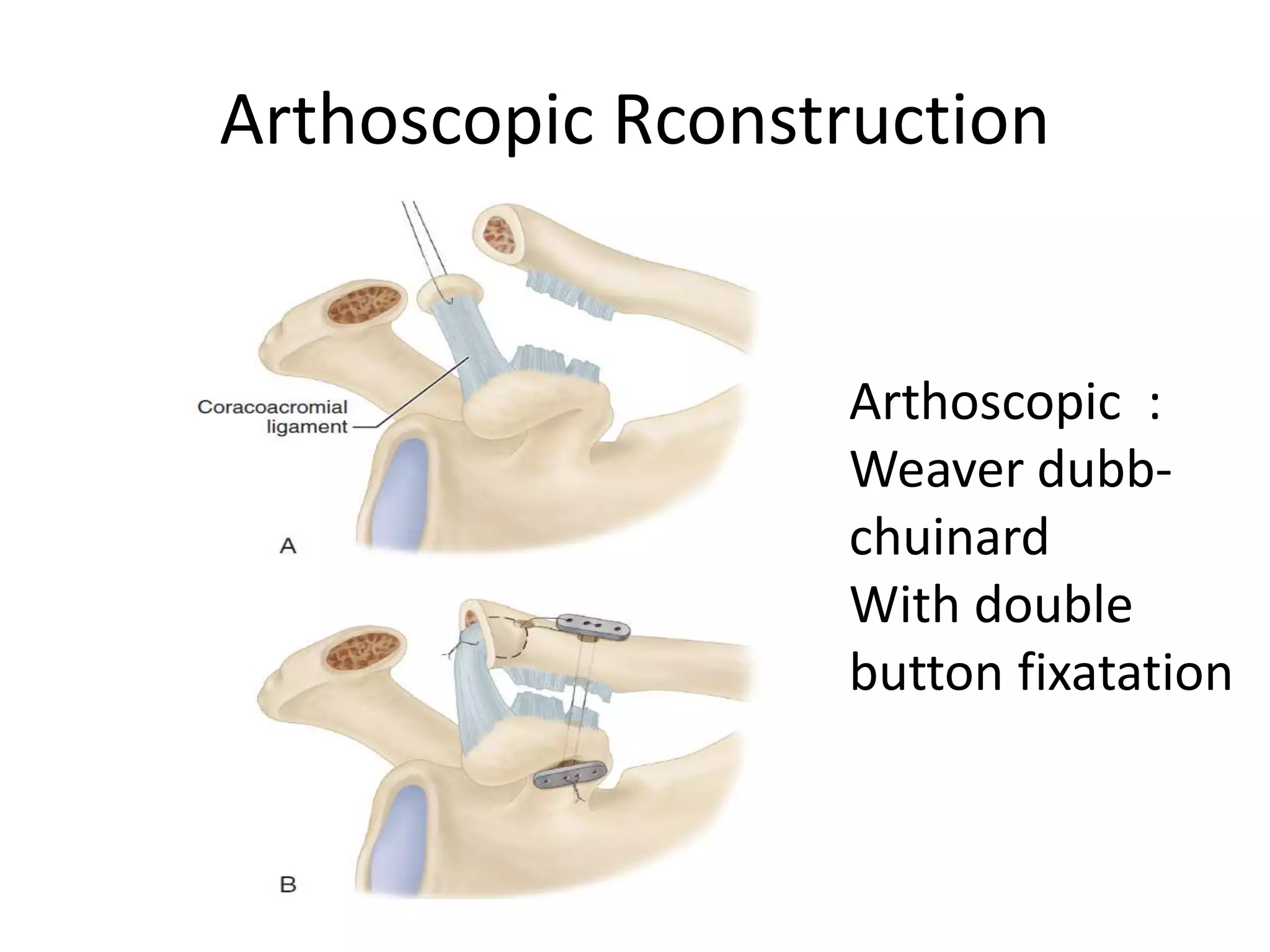
3) Non-operative treatment is usually sufficient for minor AC injuries while more severe or unstable injuries may require surgery such as ligament reconstruction or joint stabilization. Operative treatment is often needed for acute SC dislocations to reduce risk of complications.