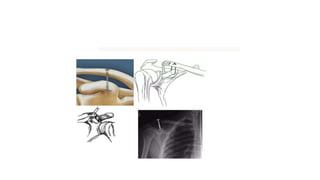
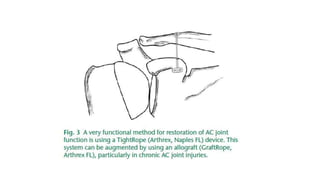
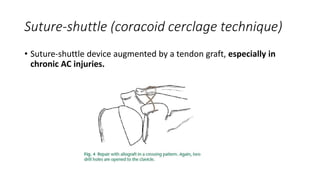
This document discusses diagnosis and treatment of acromioclavicular (AC) joint injuries. It describes the anatomy of the AC joint and classifications of injuries. For type I and II injuries, conservative treatment with slings or harnesses is recommended. Types IV, V and VI generally require surgical treatment to reduce and reconstruct injured ligaments. Recent techniques focus on arthroscopic reconstruction of the coracoclavicular ligaments and stabilization of the AC joint with suture anchors, tightropes or tendon grafts. Arthroscopy allows better visualization and less invasive reconstruction of the ligaments compared to open surgery.