APPLIED ANATOMY
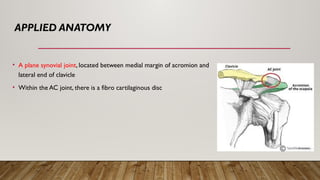
• Aplane synovial joint, located between medial margin of acromion and
lateral end of clavicle
• Within the AC joint, there is a fibro cartilaginous disc
5.
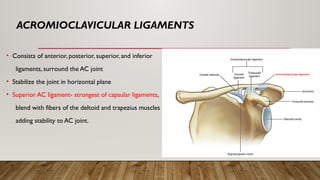
ACROMIOCLAVICULAR LIGAMENTS
• Consistsof anterior, posterior, superior, and inferior
ligaments, surround the AC joint
• Stabilize the joint in horizontal plane
• Superior AC ligament- strongest of capsular ligaments,
blend with fibers of the deltoid and trapezius muscles
adding stability to AC joint.
6.
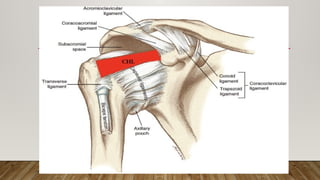
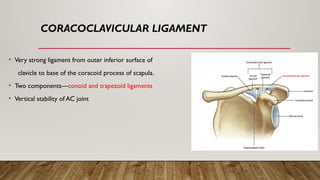
CORACOCLAVICULAR LIGAMENT
• Verystrong ligament from outer inferior surface of
clavicle to base of the coracoid process of scapula.
• Two components—conoid and trapezoid ligaments
• Vertical stability of AC joint
7.
• The onlyconnection between the upper extremity and the axial skeleton is through the clavicular
articulations at the AC and SC joints.
• SC ligaments support clavicles suspended away from the body
• CC ligament suspend upper extremities from distal clavicles
8.
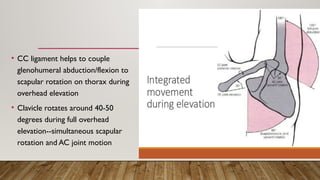
• CC ligamenthelps to couple
glenohumeral abduction/flexion to
scapular rotation on thorax during
overhead elevation
• Clavicle rotates around 40-50
degrees during full overhead
elevation--simultaneous scapular
rotation and AC joint motion
9.
OVERVIEW
• Injuries toeither AC or SC joints can result in a wide range of shoulder
dysfunction.
• Both can be injured by similar mechanisms, present with overlapping clinical
complaints, and in some cases result in injury to both locations
• Acromioclavicular injures are more common, and sternoclavicular injuries are rare
10.
RISK GROUPS
• oftenoccur in male patients less than 30 years of age
• associated with contact sports or athletic activity in which direct blow to lateral aspect of
shoulder occurs.
• The contact or collision athlete represents a “high-risk” individual (football, rugby, and
hockey)
11.
MECHANISMS OF INJURY
•Falling on an outstretched arm, locked in extension at the elbow, can drive humeral head
superiorly into acromion--low-grade AC joint injuries
• A medially directed force to lateral shoulder that drives acromion into and underneath the
distal clavicle leads to higher degrees of injury and subsequently more displacement.
12.
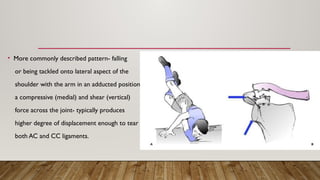
• More commonlydescribed pattern- falling
or being tackled onto lateral aspect of the
shoulder with the arm in an adducted position which produces
a compressive (medial) and shear (vertical)
force across the joint- typically produces
higher degree of displacement enough to tear
both AC and CC ligaments.
13.
• The injuryforce which drives acromion medially and downward produces a
progressive injury pattern; first disruption of AC ligaments, followed by disruption of
CC ligaments, and finally disruption of fascia overlying the clavicle that connects
deltoid and trapezius muscle attachments.
• Complete AC dislocation- the upper extremity has lost its suspensory support
from clavicle and scapula- inferior displacement of the shoulder secondary to
forces of gravity.
14.
Nontraumatic or ChronicOveruse
• AC joint arthrosis—weight lifting, laborer, repetitive overhead activity
• Repetitive low-grade AC joint injuries
• Medical cause: rheumatoid arthritis, hyperparathyroidism, scleroderma
15.
CLINICAL PRESENTATION
• Young-agedmale
• Contact or collision athlete
• H/O direct trauma
• Clinical deformity, focal tenderness and swelling
• Commonly the patient describes pain originating from the anterior-
superior aspect of the shoulder
16.
DIAGNOSIS
• Examination shouldbe in sitting or standing w/o support for the injured arm
• Check for tenderness to palpation at the AC joint and the CC interspace
• If patient can tolerate check joint for stability
• Check to see if reducible
• Examine SC joint as well
• Neurologic exam to r/o brachial plexus injury
18.
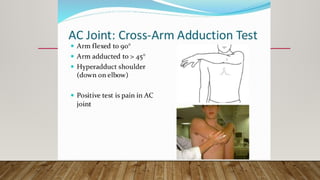
CLINICALTRIAD
• point tendernessat the AC joint,
• pain exacerbation with cross-arm adduction, and
• relief of symptoms by injection of local anesthetic agent confirm injury to the AC joint.
19.
RADIOGRAPHIC NORMAL JOINTS
•Width and configuration of AC joint in coronal plane may vary significantly from individual to individual. So, a
normal variant should not be mistaken as an injury.
• Normal width of AC joint in coronal plane is 1 to 3 mm.AC joint space diminishes with increasing age (0.5 mm in
older than 60 years is conceivably normal). Joint space of greater than 7 mm in men and 6 mm in women is
pathologic.
• Average CC distance 1.1 to 1.3 cm.An increase in CC distance of 50% over normal side signifies Complete AC
dislocation (has been seen with as little as 25% increase in CC distance).
20.
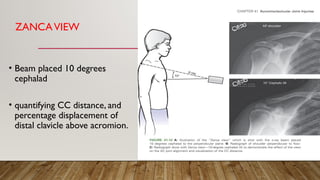
ZANCAVIEW
• Beam placed10 degrees
cephalad
• quantifying CC distance, and
percentage displacement of
distal clavicle above acromion.
21.
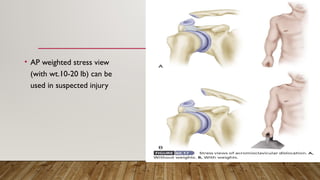
• AP weightedstress view
(with wt.10-20 lb) can be
used in suspected injury
22.
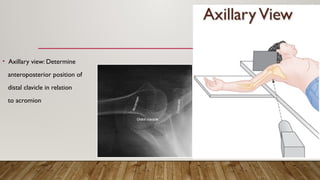
• Axillary view:Determine
anteroposterior position of
distal clavicle in relation
to acromion
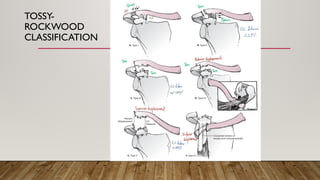
Type of InjuryClinical Features Radiological Features
Type I minimal to moderate tenderness to palpation over the AC joint
mild swelling over the AC joint
minimal pain with arm movements
respond very well to local anesthetic/ corticosteroid injections
No widening,separation or
deformity
Type II • moderate to severe tenderness with palpation of the joint
• Distal end of clavicle slightly superior to acromion
• Adduction motion of the shoulder produces pain in the AC joint
• Difficulty sleeping
• AC horizontal Instability
• Tenderness at CC space
<50% width of clavicle
displacement at AC joint
Increased CC distance < 25% of
contralateral
Type III • Upper extremity held adducted in elevated position
• shoulder droop sign
• Clavicle may be prominent enough to tent the skin.
• Moderate pain -any motion of the arm, particularly abduction
• Tenderness at AC joint, CC interspace, and along superior aspect
of lateral clavicle.
• AC joint instability in both the horizontal and vertical planes
• “shrug test” (vs typeV)
Distal clavicle Displaced
Increased CC distance 25-100% of
contralateral
May be accompanied by Fracture
coracoid > StrykerView
27.
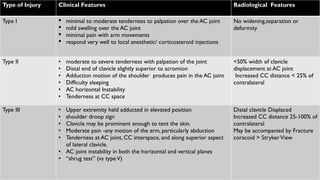
Type of
Injury
Clinical FeaturesRadiological Features
Type IV • All clinical findings of type III injury.
• clavicle is translated posteriorly compared with uninjured
shoulder may be “buttonholed” through trapezius muscle
and tents posterior skin.
• AC joint cannot be reduced manually
• Examine SC joint “bipolar” or “floating clavicle” injuries,
Best Observed in AxillaryView
Lateral clavicle displaced posterior through
trapezius
TypeV • Distal end of clavicle grossly superiorly displaced, tenting
the skin
• Downward Displacement of Upper Extremity
• More Pain than Type III secondary to more soft tissue
disruption.
• Shoulder musculature becomes weak secondary to disuse
or as part of the injury pattern-scapular dyskinesis
ZancaView
Increased CC distance > 100% of
contralateral
TypeVI • superior aspect of shoulder has flat appearance
• acromion is prominent
• associated fractures of clavicle,upper ribs or injury to upper
roots of brachial plexus
• Mechanism :Severe Hyperabduction and ER + retraction of
scapula
Subacromial type - decreased CC distance,
distal clavicle in subacromial location.
Subcoracoid type - reversed CC distance,
clavicle displaced inferior to coracoid process
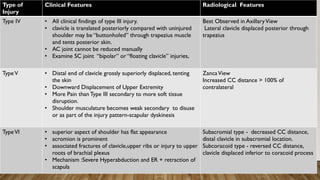
29.
• Children andadolescents may sustain a variant of complete
AC dislocation (most often Salter–Harris type I or II)
• Radiographs reveal displacement of distal clavicular
metaphysis superiorly (through a dorsal rent in periosteal
sleeve) with increase in CC interspace. Epiphysis and intact
AC joint remain in their anatomic locations
30.
TREATMENT GOALS
• Pain-freeshoulder movement in a range-of-motion arc approaching
normal
• Unimpaired daily activities
DURING 1ST WEEKOFTREATMENT
• Immobilization device (Arm slings, adhesive tape strappings, braces and plaster)-
To support the weight of upper extremity and reduce the stress placed upon the injured
ligaments
• Ice and analgesics
To reduce pain and inflammation
33.
AFTER 1 TO2 WEEKS
• Strengthening exercises commenced with particular focus on periscapular muscles
that are important to shoulder biomechanics.
• Heavy stresses, lifting, and contact sports should be delayed until there is full range
of motion and no pain to joint palpation.This process can take up to 2 to 4 weeks
34.
DISADVANTAGES OF NONOPERATIVE
TREATMENT
• SKIN PRESSURE AND ULCERATION
• RECURRENCE OF DEFORMITY
• WEARING A BRACE FOR LONG TIME(8 WEEKS)
• POOR PATIENT COOPERATION
• INTERFERENCE WITH DAILY ACTIVITIES
• LOSS OF SHOULDER AND ELBOW MOTION
• SOFT TISSUE CALCIFICATIONS
• LATE ACROMIOCLAVICULAR ARTHRITIS
• LATE MUSCULAR ATROPHY,FATIGUE AND WEAKNESS.
35.
TYPE III- OPERATIVEOR NONOPERATIVE ?
• In prospective randomized studies between operative and nonoperative treatment of type III AC joint
injuries, patients treated nonoperatively demonstrated a quicker return of function and sustained
fewer complications than patients treated operatively.
• Patients treated conservatively returned to work on average 2.1 weeks from injury and the strength
and ROM of the injured shoulder were comparable to the contralateral uninjured shoulder with a
mean follow-up of 2.6 years (Wojtys and Nelson)
• Operatively treated AC injuries showed a significantly higher incidence of osteoarthritis and CC
ligament ossification
• A proportion of conservatively treated patients will have persistent pain and inability to return to
their sport or job. Subsequent surgical stabilization has allowed return to sport or work in such cases
36.
Reasons for lower-gradeAC joint injuries being symptomatic –
• posttraumatic arthritis
• posttraumatic osteolysis of the distal clavicle,
• recurrent AP subluxation,
• torn capsular ligaments trapped within the joint,
• loose pieces of articular cartilage,
• detached intra-articular meniscus or associated intra-articular fracture
fragment.
37.
CHRONIC ACROMIOCLAVICULAR INJURIES
•Chronic pain after type I and II injuries - NSAIDS, avoidance of painful activity or positions, and intra-articular
injection with corticosteroid
• Type I-
Operative excision of distal clavicle (limited to less than 10 mm )-open or arthroscopic
• Type II-
Distal clavicle excision + AC capsular reconstruction or coracoacromial ligament transfer
• Chronic pain and instability after types III, IV, andV- Distal clavicle excision + Transfer of acromial attachment of
coracoacromial ligament to the resected surface of distal clavicle and concurrent CC stabilization
38.
OPERATIVETREATMENT
Indications -
• Patients(types I,II,III) who have failed a minimum 6 weeks of shoulder stabilization–directed physical therapy
(delayed surgical reconstruction using a tendon graft)
• Active healthy patients with complete AC joint injuries (types IV,V, andVI)- significant morbidity associated
with the injury pattern- persistently dislocated, unstable AC joint, with change in scapular kinematics, and
shoulder dysfunction.
• Fracture of coracoid extending intra-articularly into glenoid (5 mm or more of glenoid displacement )
39.
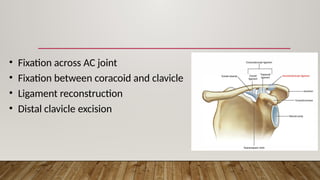
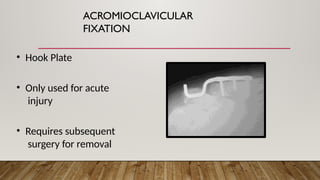
• Fixation acrossAC joint
• Fixation between coracoid and clavicle
• Ligament reconstruction
• Distal clavicle excision
40.
ANY SURGICAL PROCEDUREFOR AC JOINT
DISLOCATION SHOULD FULFILLTHREE REQUIREMENTS
• AC JOINT MUST BE EXPOSED AND DEBRIDED
• CC AND AC LIGAMENTS MUST BE REPAIRED OR
RECONSTRUCTED
• STABLE REDUCTION OF THE AC JOINT MUST BE OBTAINED
Achieving these three goals , no matter how the joint is fixed , should give
acceptable results.
41.
DISADVANTAGES OF
SURGICAL
MANAGEMENT
• INFECTION
•HEMATOMA FORMATION
• ANAESTHETIC RISK
• SCAR FORMATION
• RECURRENCE OF DEFORMITY
• METAL BREAKAGE, LOOSENING,MIGRATION
• SECOND SURGERY FOR REMOVAL
• BREAKAGE OR LOOSENING OF SUTURES
• EROSION OR FRACTURE OF DISTAL CLAVICLE
• LATE ARTHRITIS AND LOSS OF JOINT MOTION.
FIXATION BETWEEN CORACOID
ANDCLAVICLE
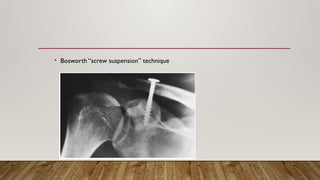
• Bosworth popularized the use of a screw for fixation of the
clavicle to the coracoid
• This technique initially did not include recommendation for
repair or reconstruction of the CC ligaments
• Today the use of screws and suture loops has been described
alone and in combo with ligament reconstruction
• Placement of synthetic loops between the coracoid and
clavicle can be done arthroscopically, main advantage: doesn’t
require staged screw removal
LIGAMENT RECONSTRUCTION
• Weaverand Dunn were the 1st to describe transfer for the native CA
ligament to reestablish AC joint stability
• Their technique described excision of the distal clavicle with this ligament
transfer
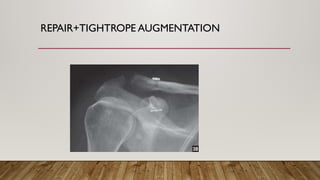
• Construct can be augmented with a suture loop for protection until the
transferred ligament heals
Open or Arthroscopy
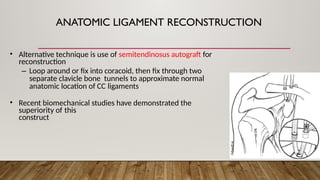
ANATOMIC LIGAMENT RECONSTRUCTION
•Alternative technique is use of semitendinosus autograft for
reconstruction
– Loop around or fix into coracoid, then fix through two
separate clavicle bone tunnels to approximate normal
anatomic location of CC ligaments
• Recent biomechanical studies have demonstrated the
superiority of this
construct
Fractures
• lateral claviclefracture
• base or neck of coracoid process fracture
• concomitant injury to medial clavicular epiphysis (less than 30 years of age)
• Fracture of midshaft of clavicle with either anterior or posterior subluxation/dislocation
of SC joint (uncommon)
53.
SECONDARY OSTEOARTHRITIS
• latecomplication
• usually be managed conservatively,
• If pain is marked, the outer 2 cm of clavicle can be excised.
54.
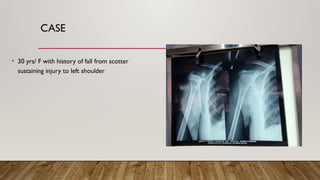
CASE
• 30 yrs/F with history of fall from scotter
sustaining injury to left shoulder
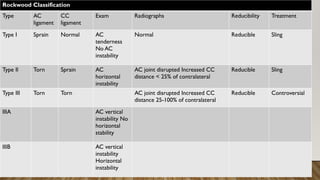
Rockwood Classification
Type AC
ligament
CC
ligament
ExamRadiographs Reducibility Treatment
Type I Sprain Normal AC
tenderness
No AC
instability
Normal Reducible Sling
Type Il Torn Sprain AC
horizontal
instability
AC joint disrupted Increased CC
distance < 25% of contralateral
Reducible Sling
Type III Torn Torn AC joint disrupted Increased CC
distance 25-100% of contralateral
Reducible Controversial
IIIA AC vertical
instability No
horizontal
stability
IIIB AC vertical
instability
Horizontal
instability
58.
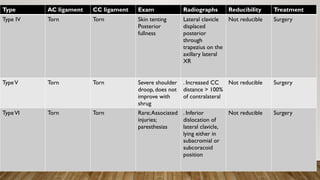
Type AC ligamentCC ligament Exam Radiographs Reducibility Treatment
Type IV Torn Torn Skin tenting
Posterior
fullness
Lateral clavicle
displaced
posterior
through
trapezius on the
axillary lateral
XR
Not reducible Surgery
TypeV Torn Torn Severe shoulder
droop, does not
improve with
shrug
. Increased CC
distance > 100%
of contralateral
Not reducible Surgery
TypeVI Torn Torn Rare;Associated
injuries;
paresthesias
. Inferior
dislocation of
lateral clavicle,
lying either in
subacromial or
subcoracoid
position
Not reducible Surgery
59.
REFERENCES
• Rockwood andGreens Fractures in Adult, Ninth edition
• Campbell Orthopaedics ,14th
edition
• Apley and Solomon’s System of Orthopaedics andTrauma,Tenth Edition
• https://www.orthobullets.com/shoulder-and-elbow/3047/acromioclavicular-joint-injury
#6 conoid ligament, the more medial of the two ligaments, is cone shaped, with the apex of the cone attaching on the posteromedial side of the base of the coracoid process. The base of the cone attaches onto the conoid tubercle on the posterior undersurface of the clavicle.
#19 In a study of 100 radiographs of normal shoulders, Urist found that
49% of the AC joints were inclined superolateral to inferomedial, with articular surface of clavicle overriding acromion;
27% were vertical
3% were inclined superomedial to inferolateral, with the articular surface of clavicle underriding acromion
21% were incongruent, with clavicle lying either superior or inferior to acromial articular surface.
#25 Based on anatomic severity of the injury.
III- Radiographic findings include a 25–100% increase in the coracoclavicular space in comparison to the normal shoulder
V- increased greater than 100%, stripping of deltotrapezial fascia
#35 Controversy-Several studies advocate operative management over nonoperative based on functional outcome, while other recommend conservative. But the auther of rockwood recommend nonoperative
#36 Surgical management may be indicated in such conditions
#46 Obsolete- fixation failure, loss of reduction, and disastrous migration of hardware
#49 Resections should be limited to less than 10 mm of distal clavicle as to limit the disruption of the superior and posterior capsular/ligament structures .
Attached by transosseous sutures
#51 brachial plexus neurapraxia after sustaining a type III AC separation. The patient responded well to CC stabilization.
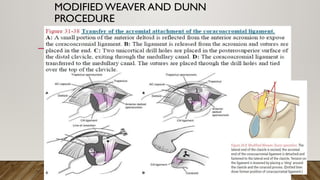
Coracoclavicular Ossification -intrinsic healing response within this area following injury to the CC ligaments. Usually, it has no effect on the functional outcome but if present may require removal to facilitate full reduction of the AC joint and CC distance at the time of operative intervention.
Osteolysis of the Distal Clavicle -a radiographic finding, due to repeated microtrauma with a recurrent inflammatory process following low-grade AC separations
Scapulothoracic Dissociation -lateral displacement of the scapula resulting in a traction injury to the neurovascular structures of the shoulder
#53 The patient will be aware of some weakness during strenuous overarm activities and pain is often not completely abolished





















































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)
