Download as ODP, PPTX


![Risk level (P*S) and (D)
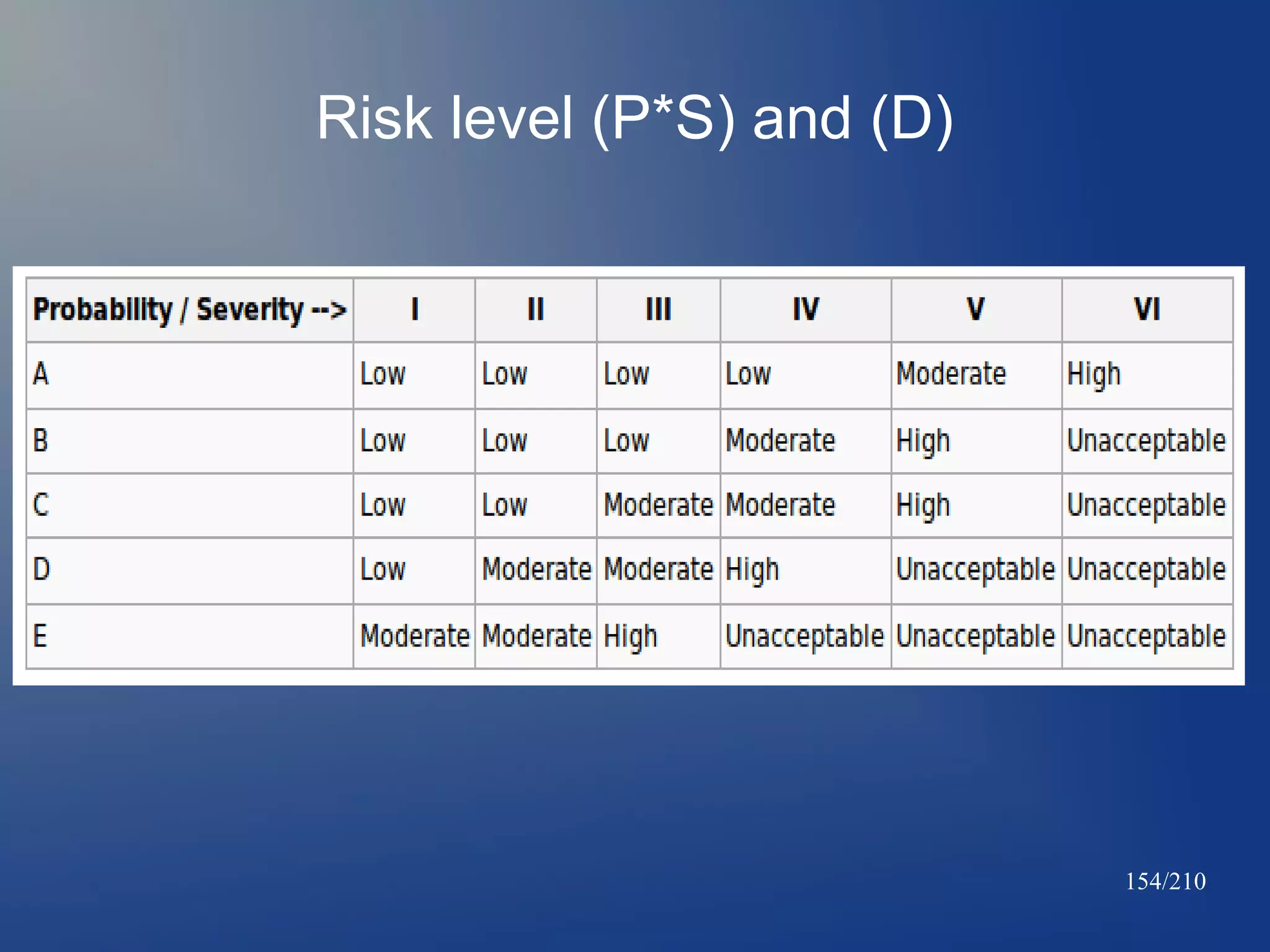
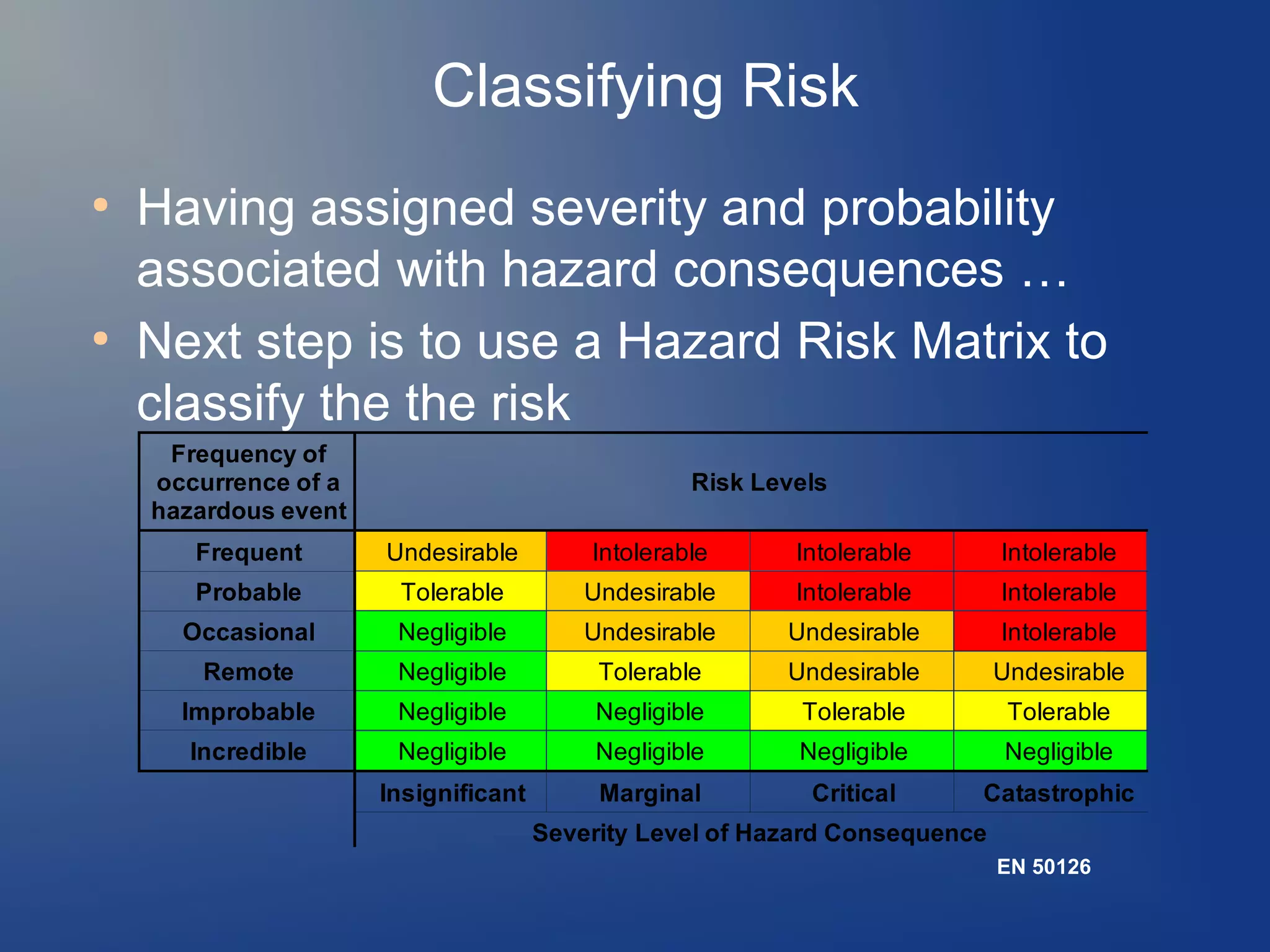
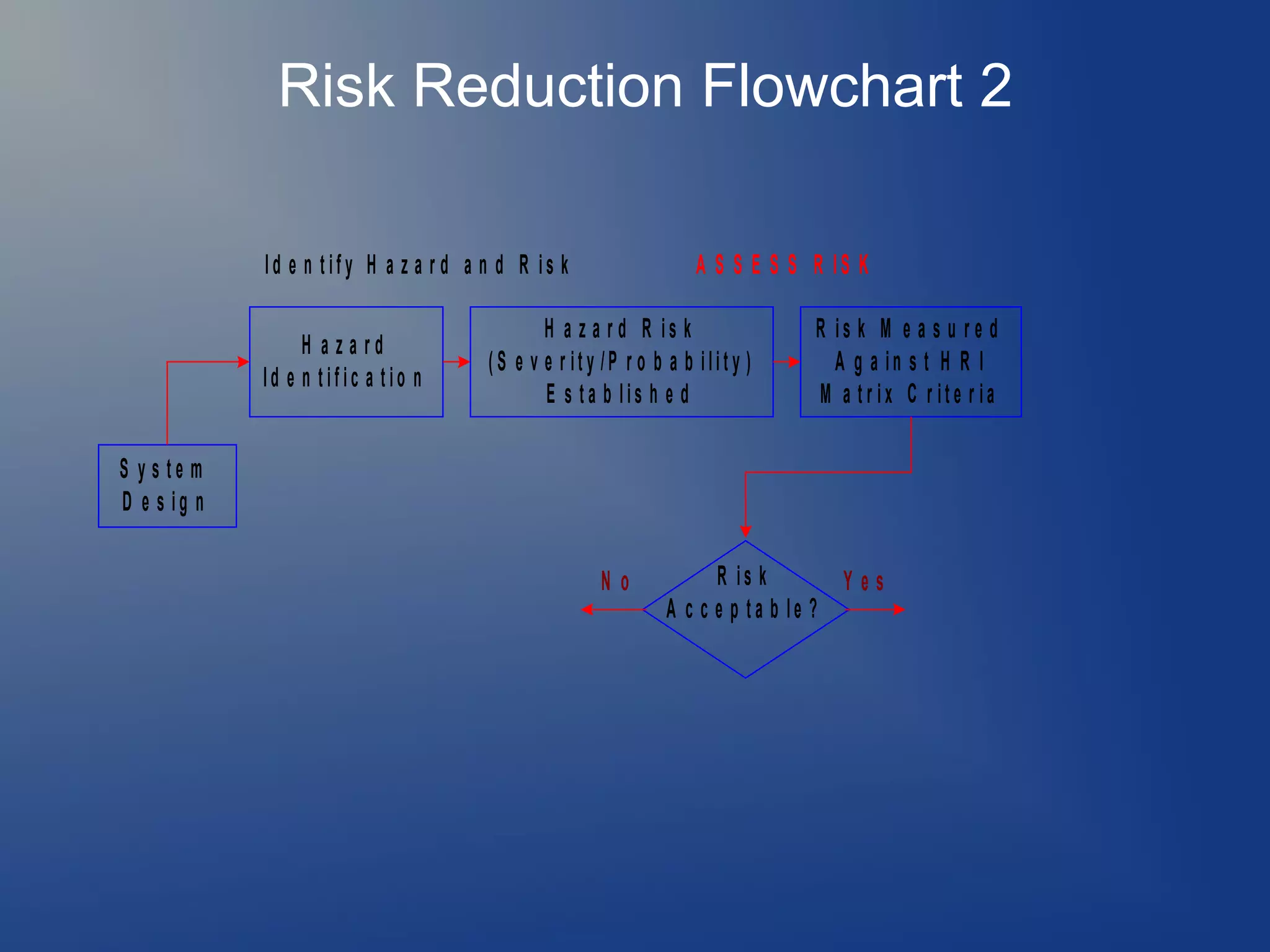
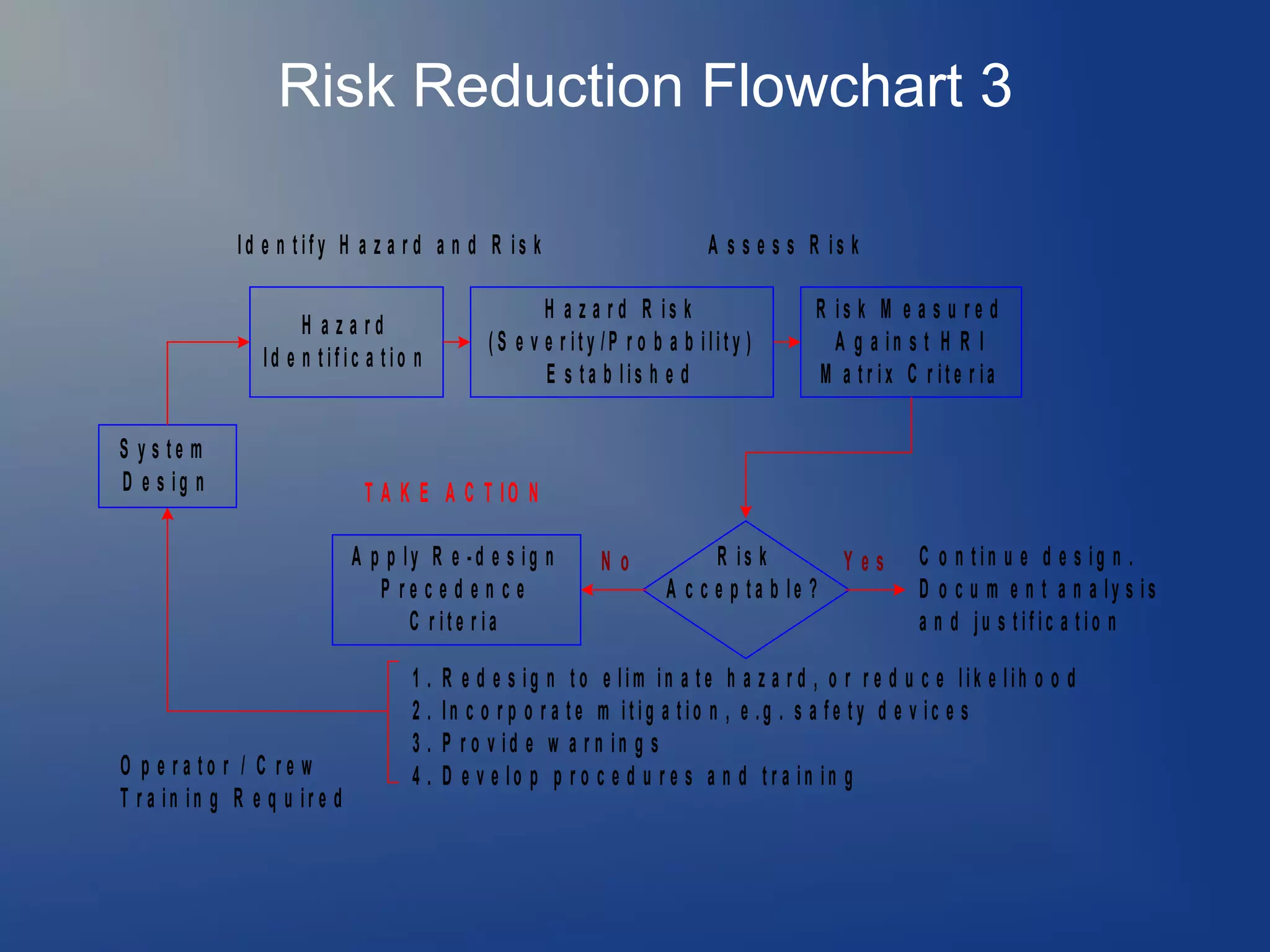
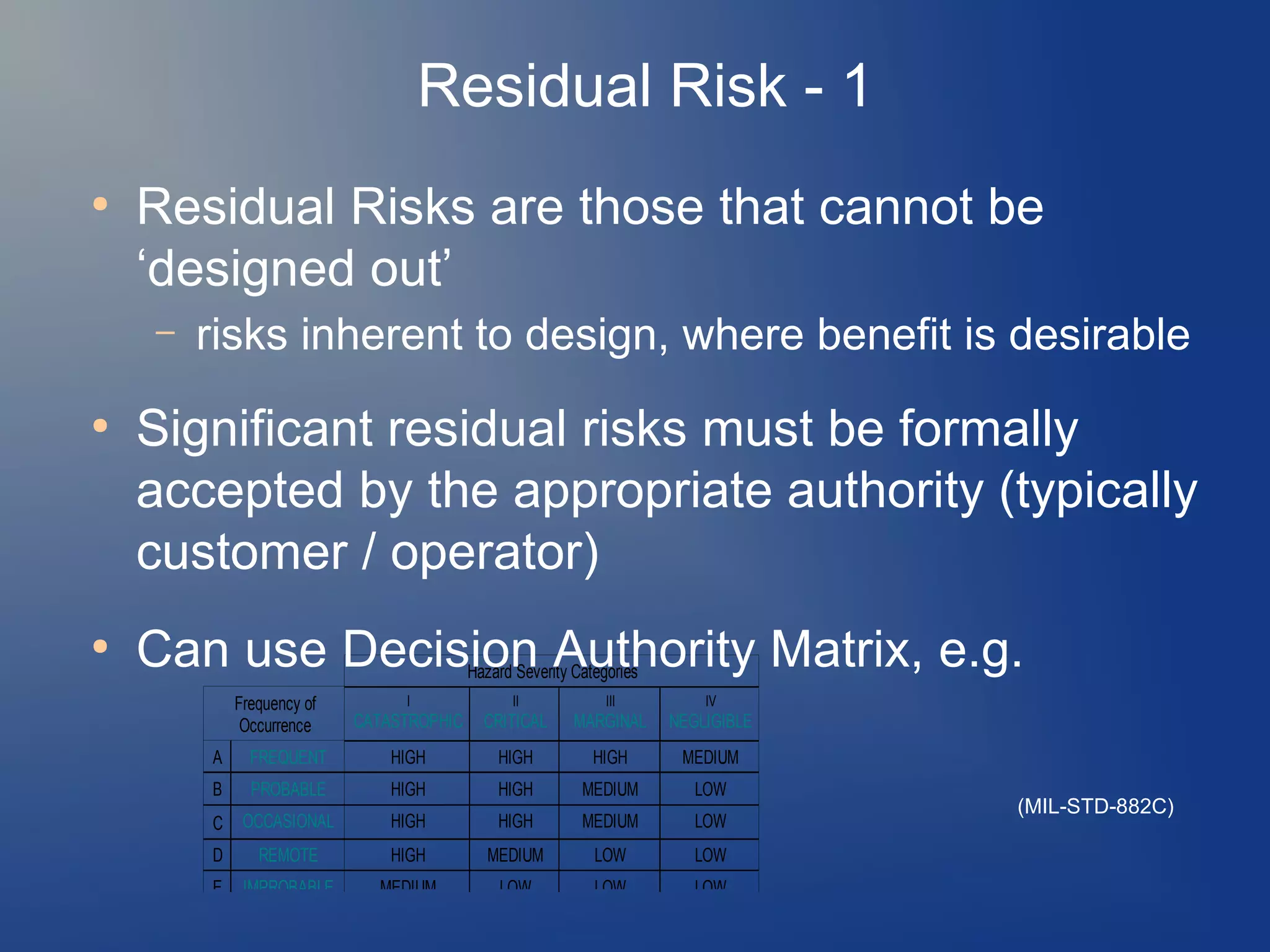
Preliminary Risk levels can be selected based on a Risk
Matrix like shown below, based on Mil. Std. 882.[24] The
higher the Risk level, the more justification and mitigation is
needed to provide evidence and lower the risk to an
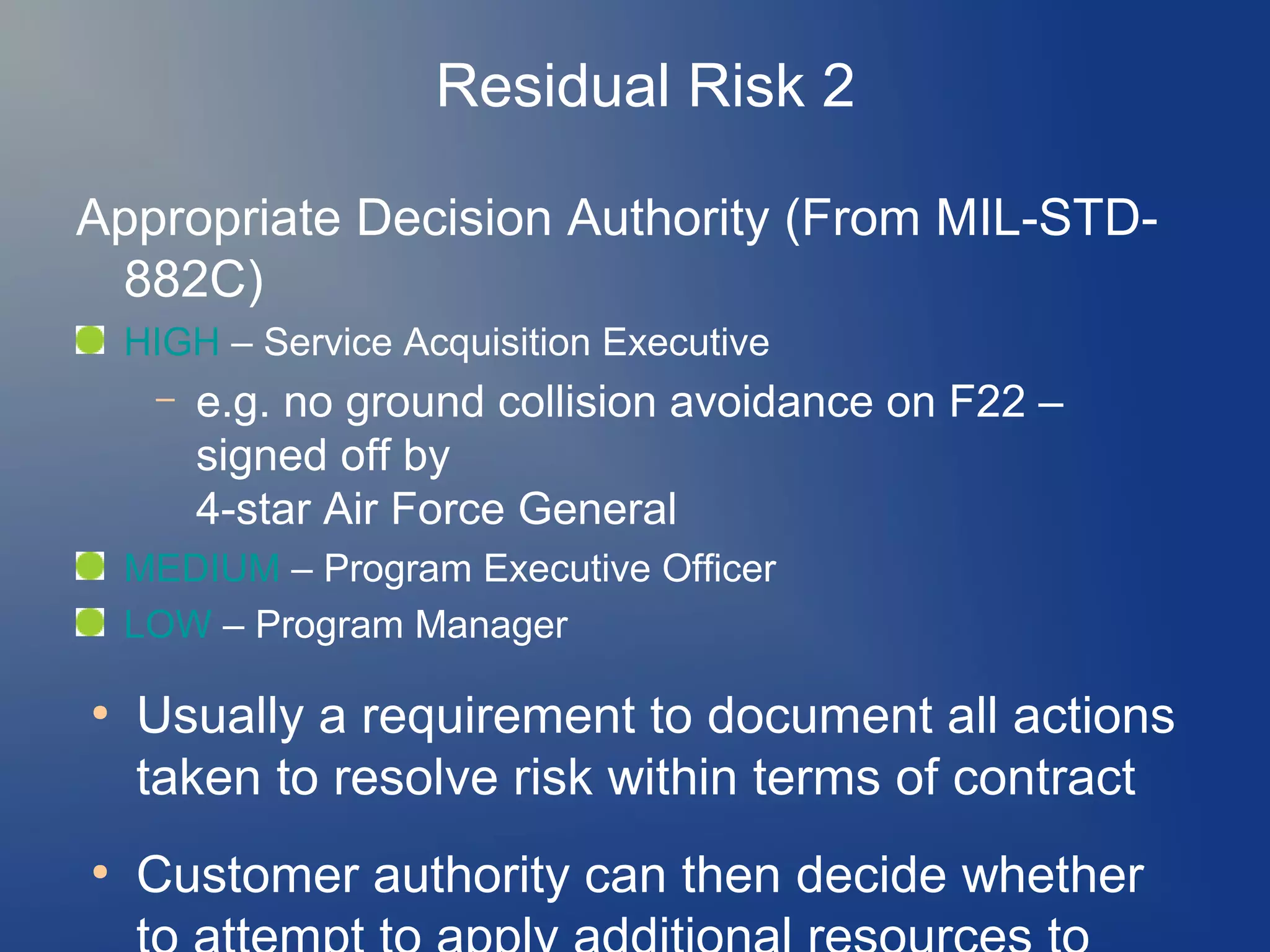
acceptable level. High risk should be indicated to higher
level management, who are responsible for final decision
making.
153/210](https://image.slidesharecdn.com/accidentinvestigationcourse210slides28dec2013-1-140105002810-phpapp01/75/Accident-investigation-course-153-2048.jpg)









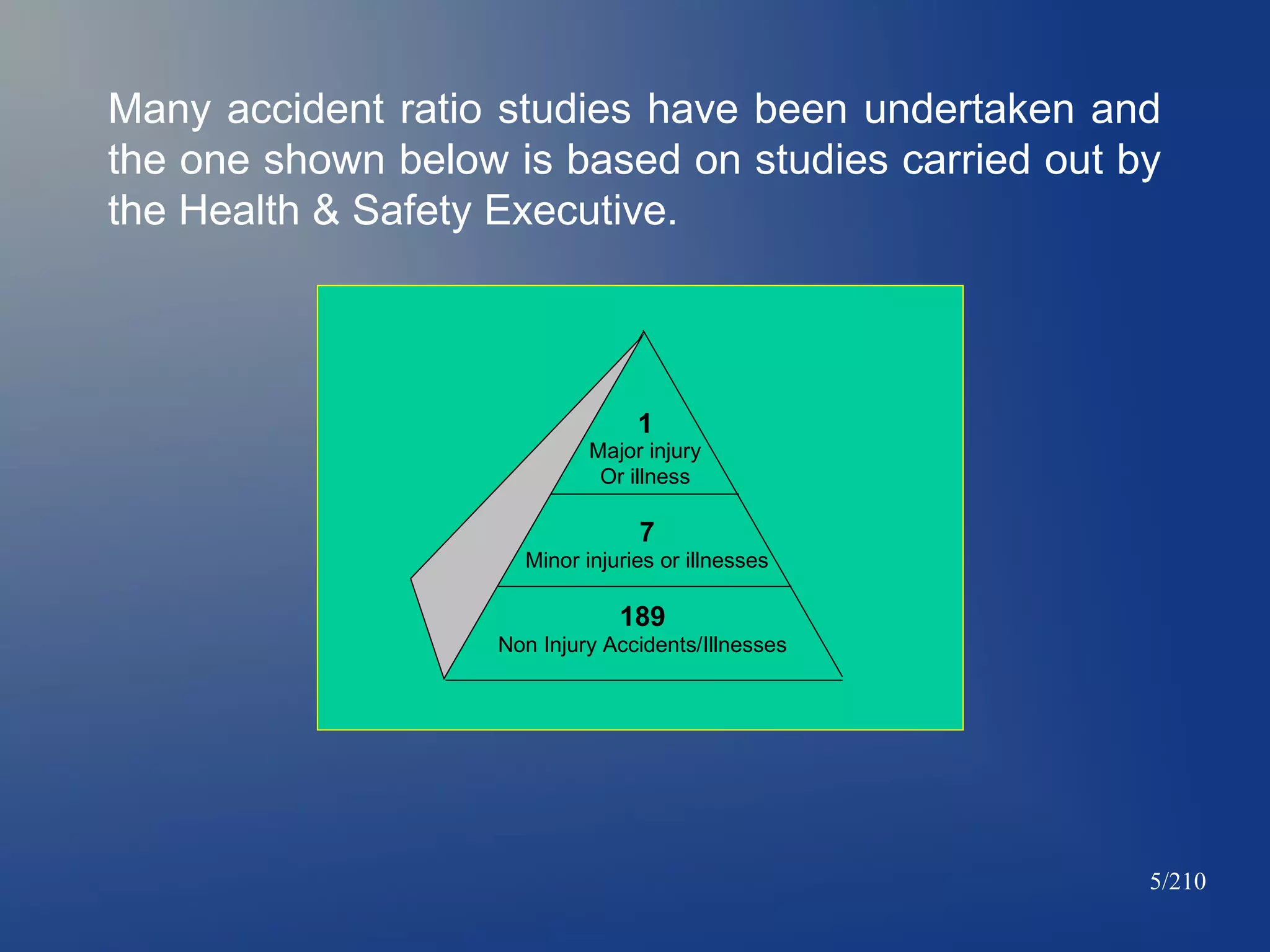
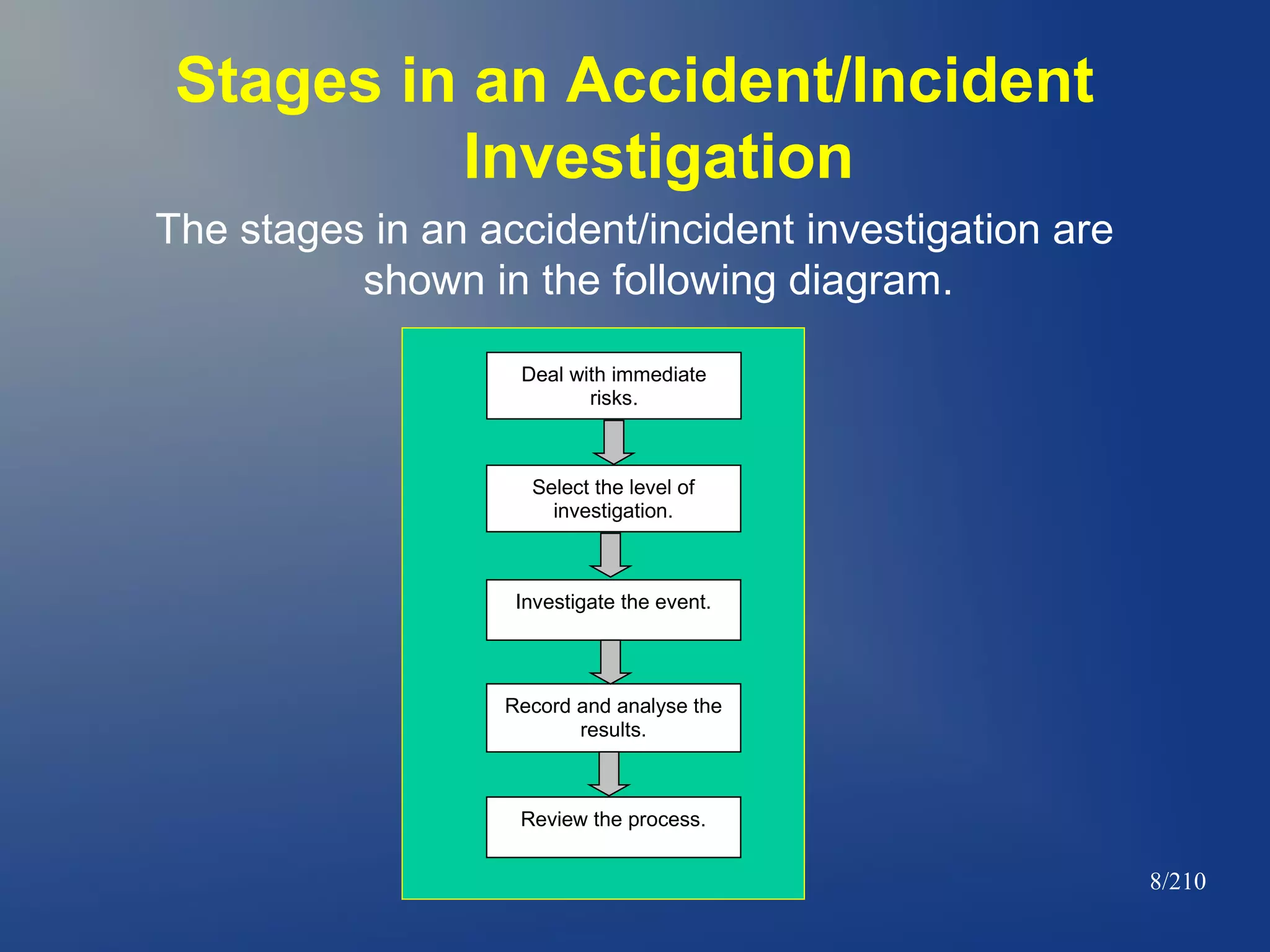
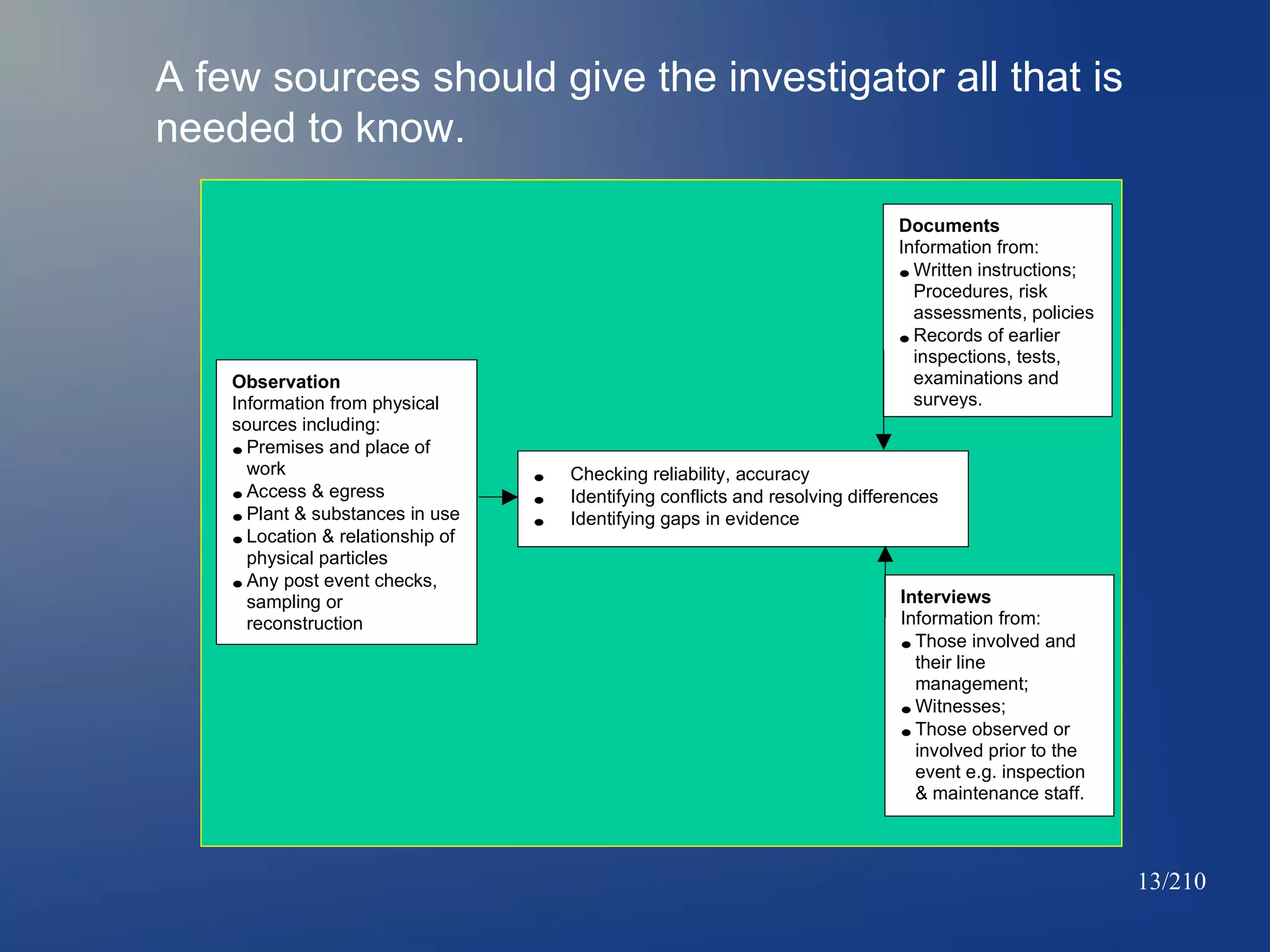
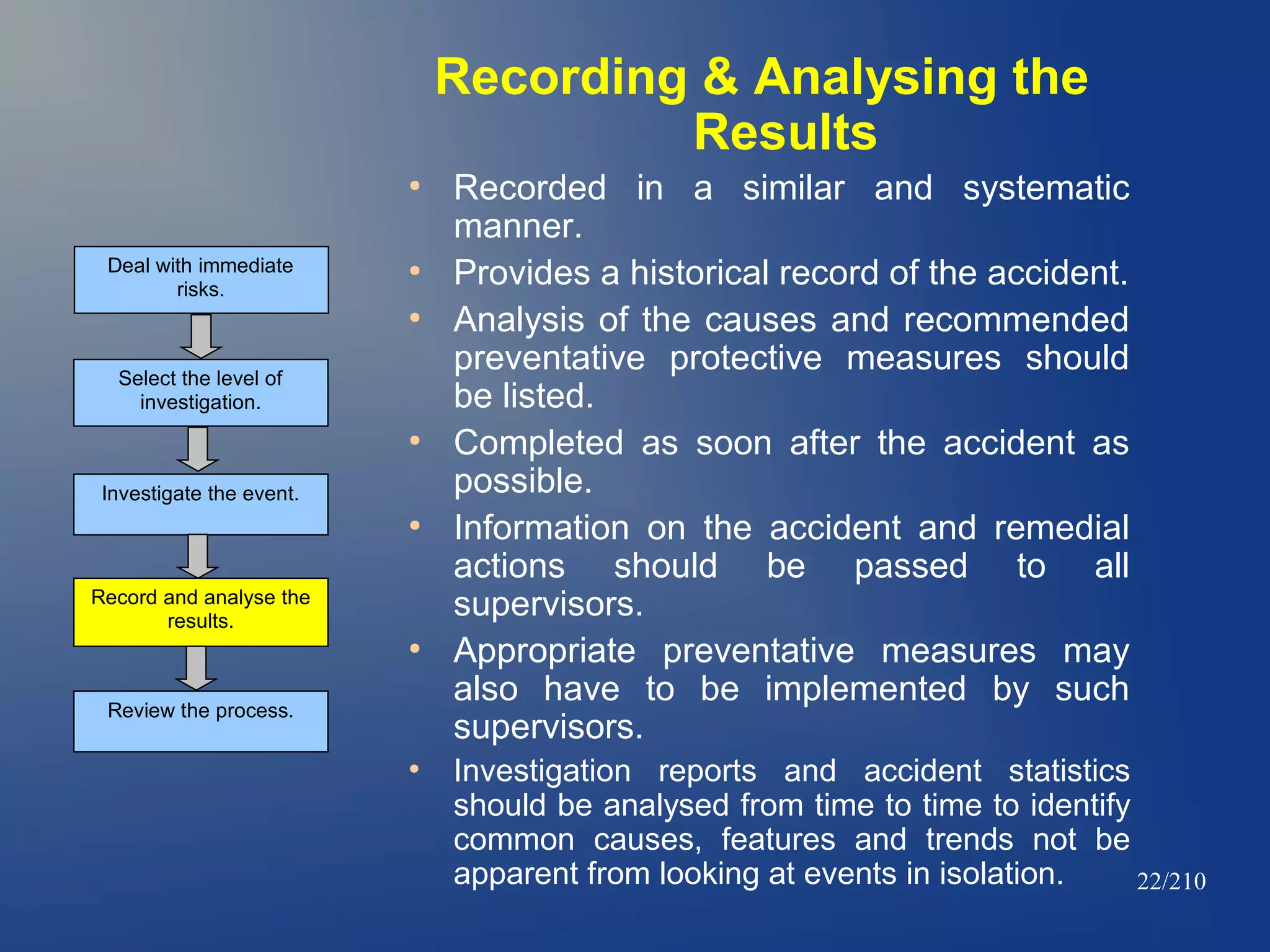
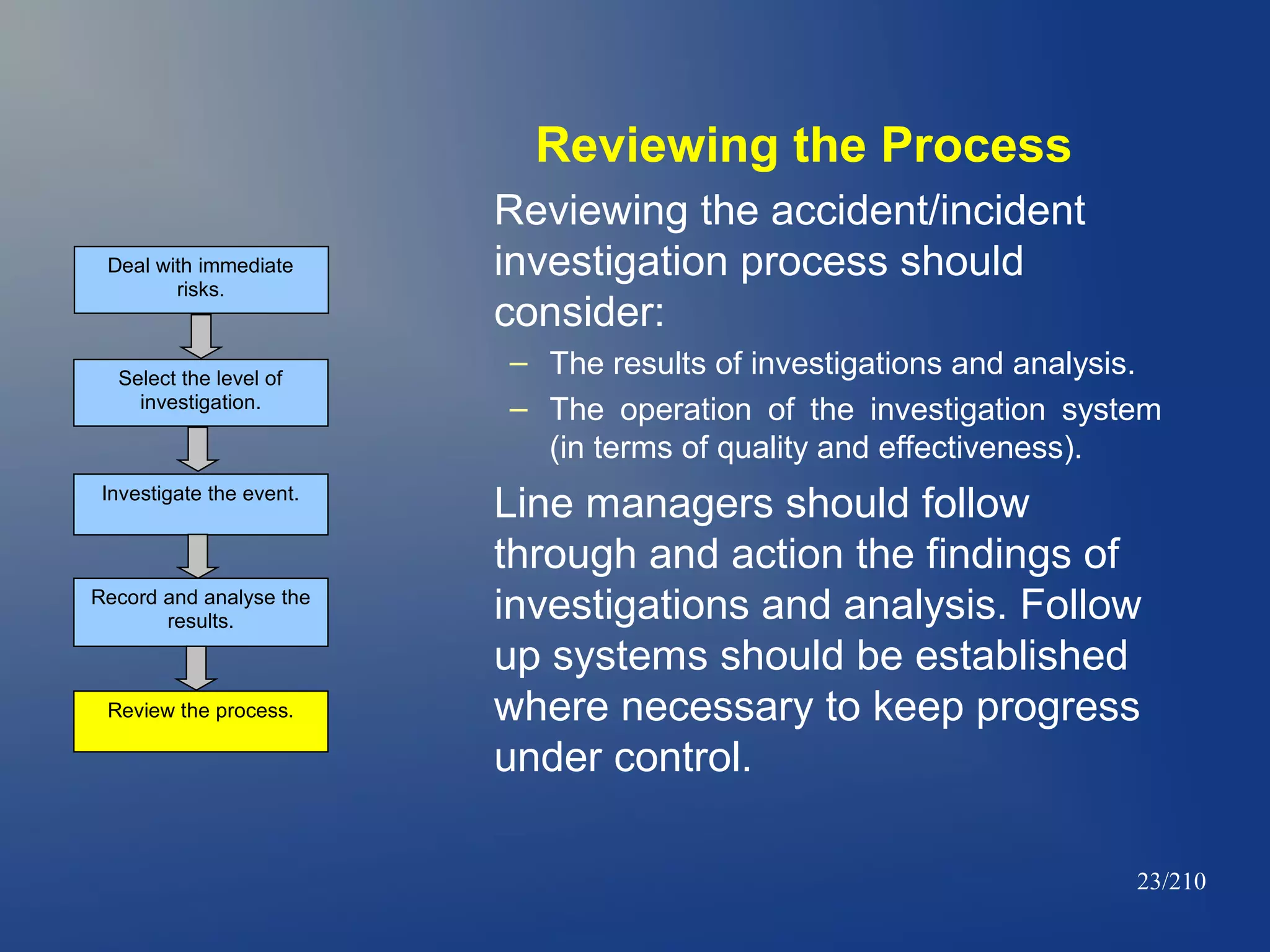
This document outlines the process for investigating accidents and incidents. It defines an accident investigation as an important part of a safety management system that highlights why accidents occur and how to prevent them. The primary goals of an investigation are to identify the immediate and root causes of events and implement remedies to improve safety. All accidents, regardless of severity, should be investigated to some degree to identify common causes and trends. The stages of an investigation include dealing with immediate risks, selecting an investigation level, investigating the event, recording and analyzing results, and reviewing the process. Thorough observation, documentation review, and interviews are important for determining causes. Remedial actions should follow a hierarchy of risk control from elimination to engineering to administrative controls.





































































































