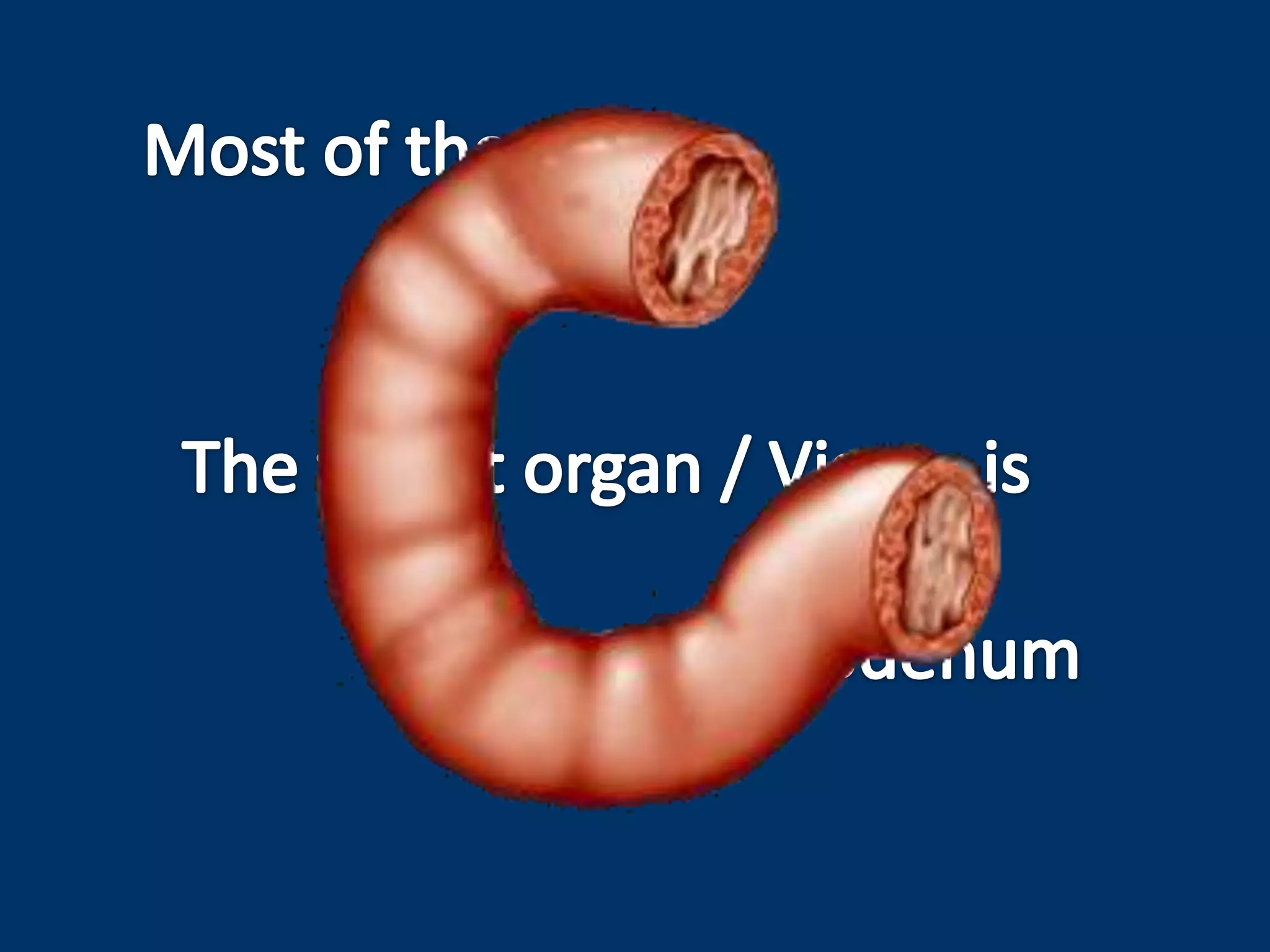
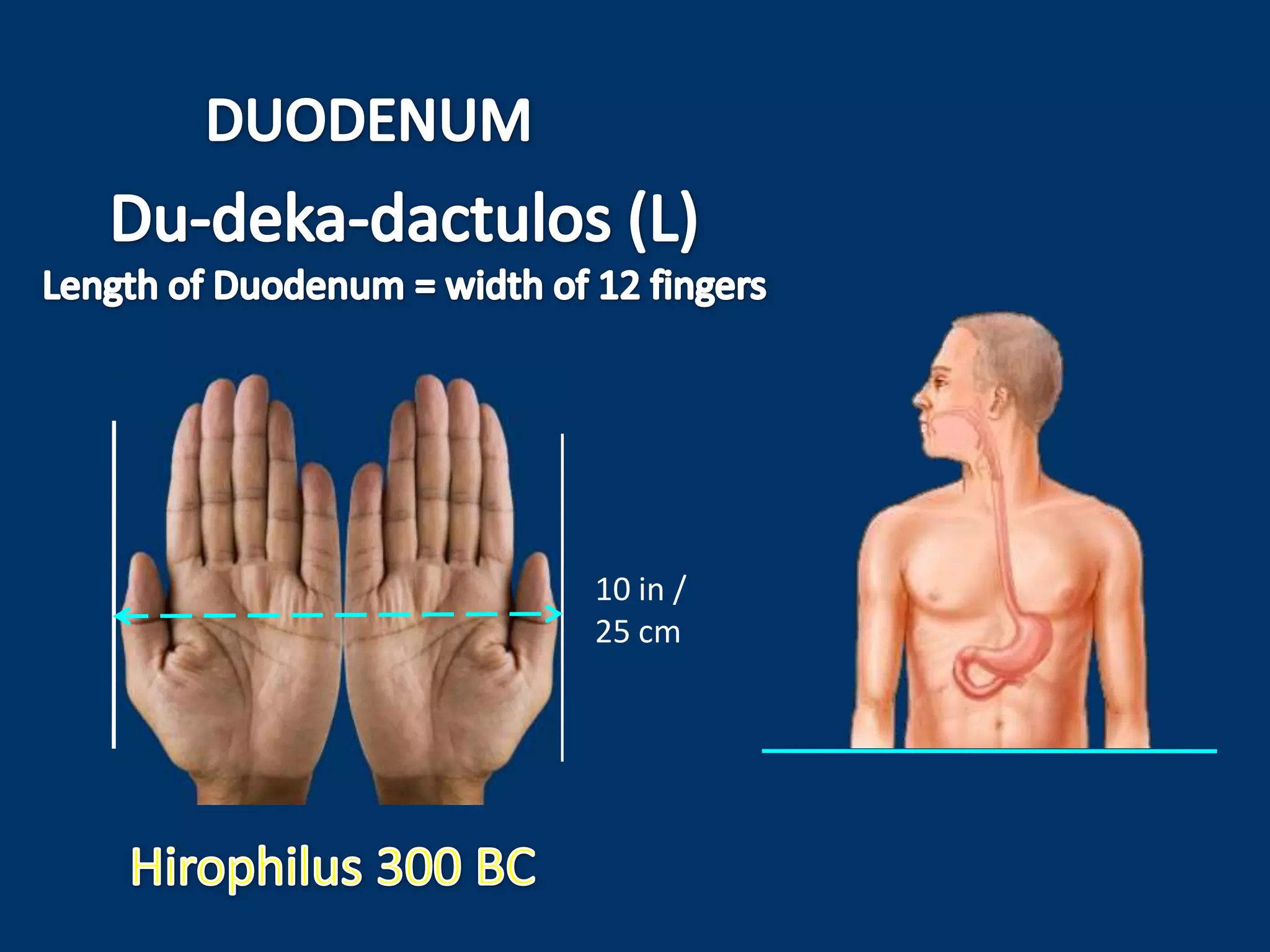
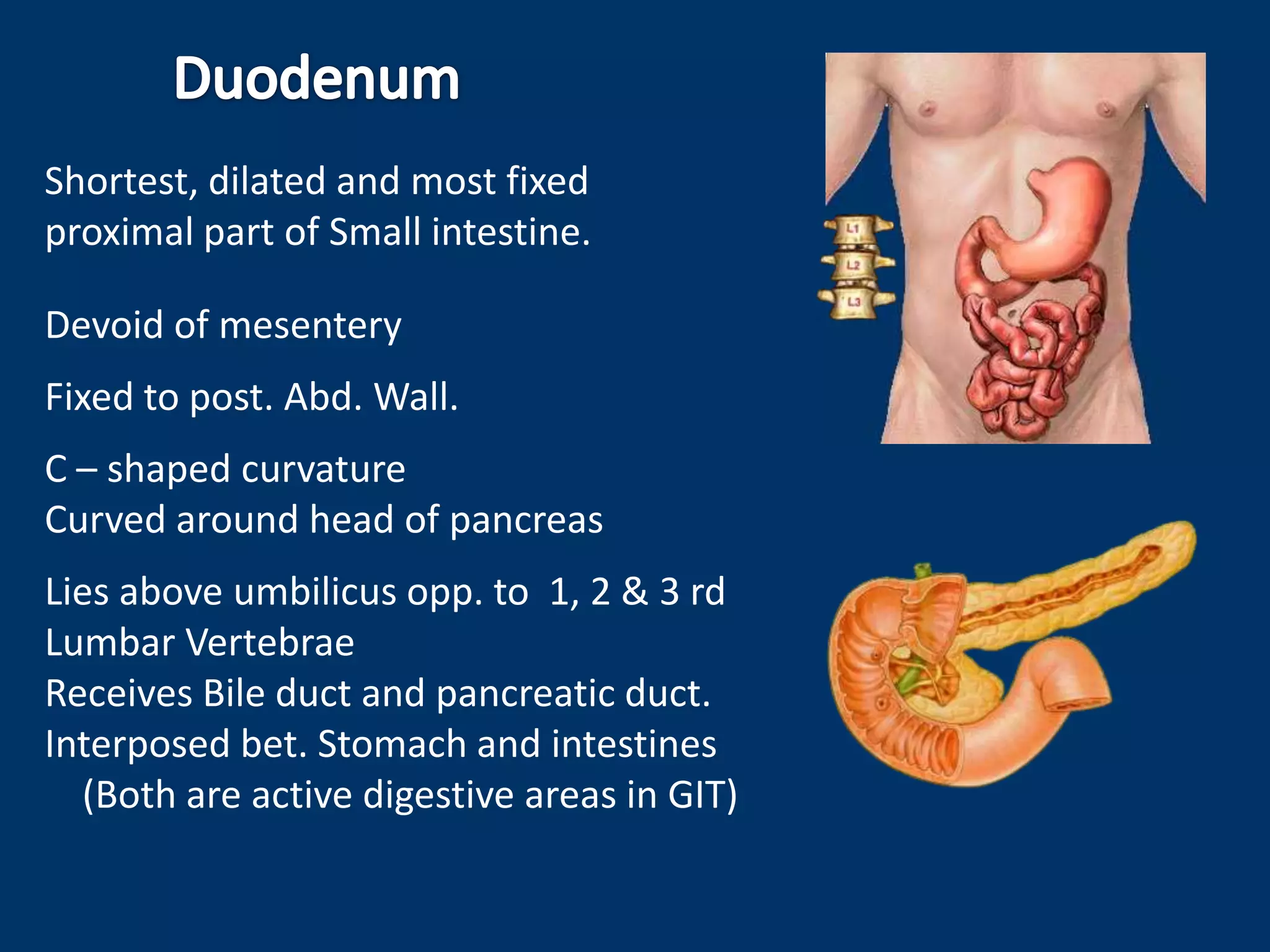
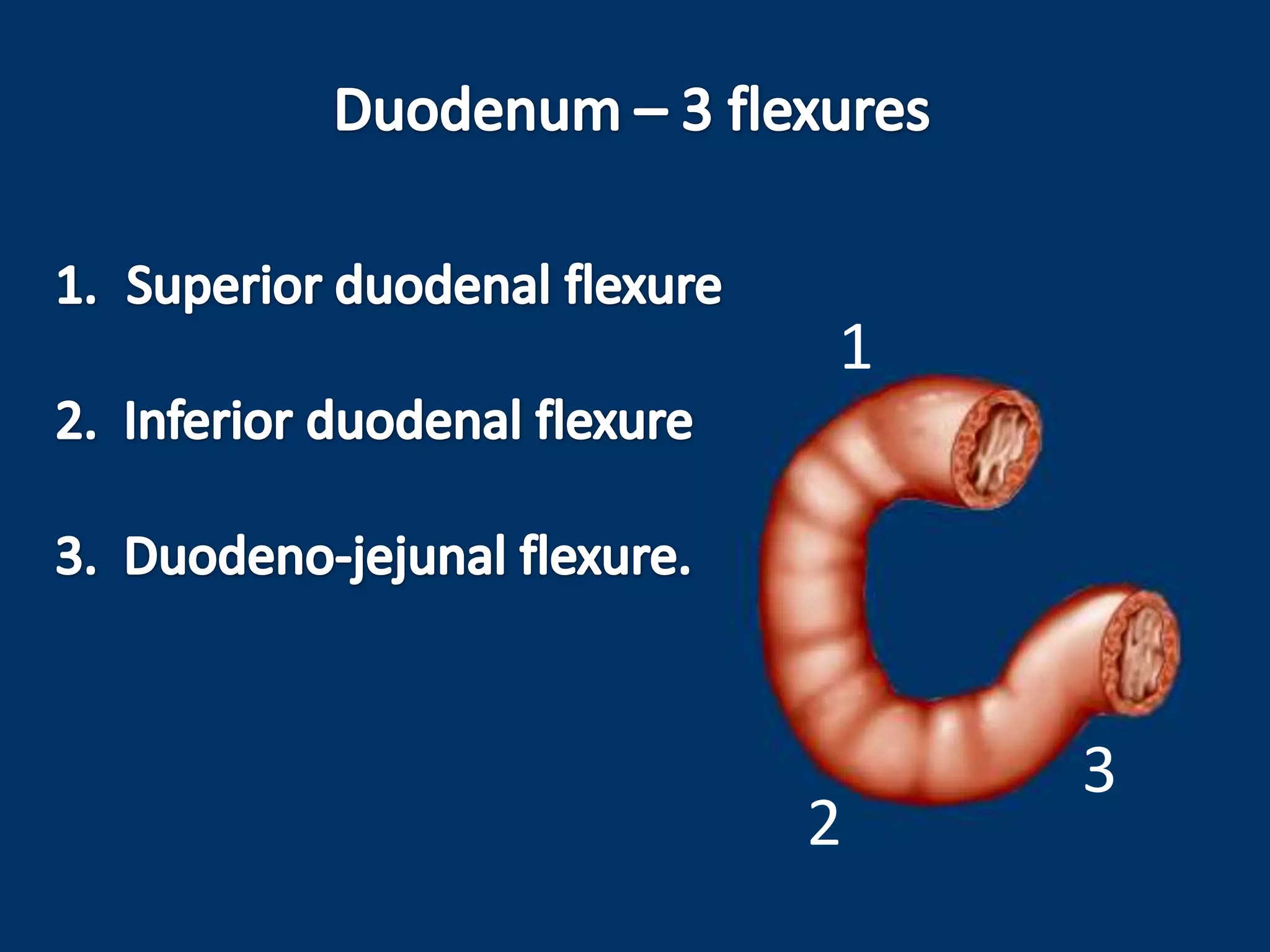
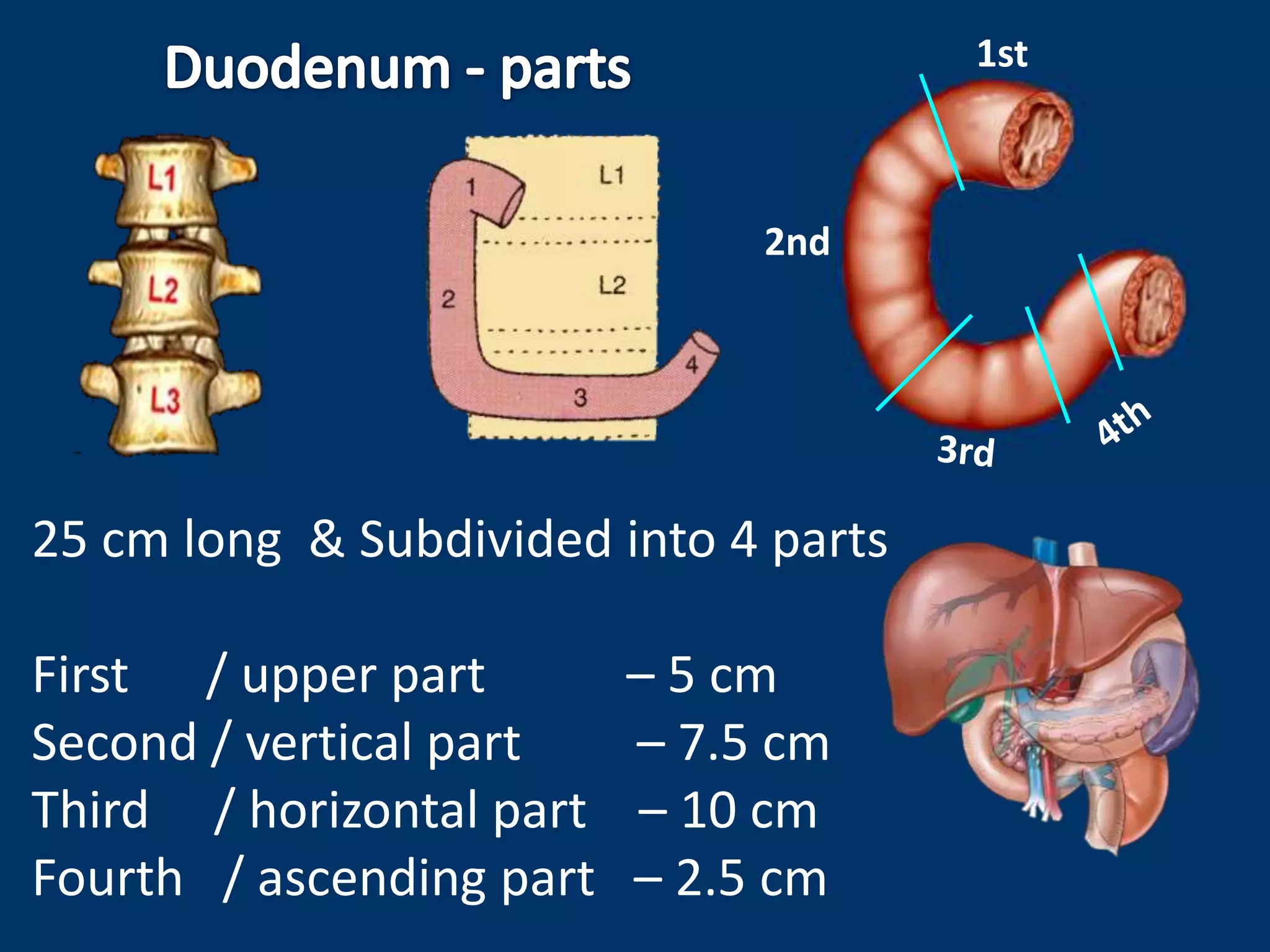
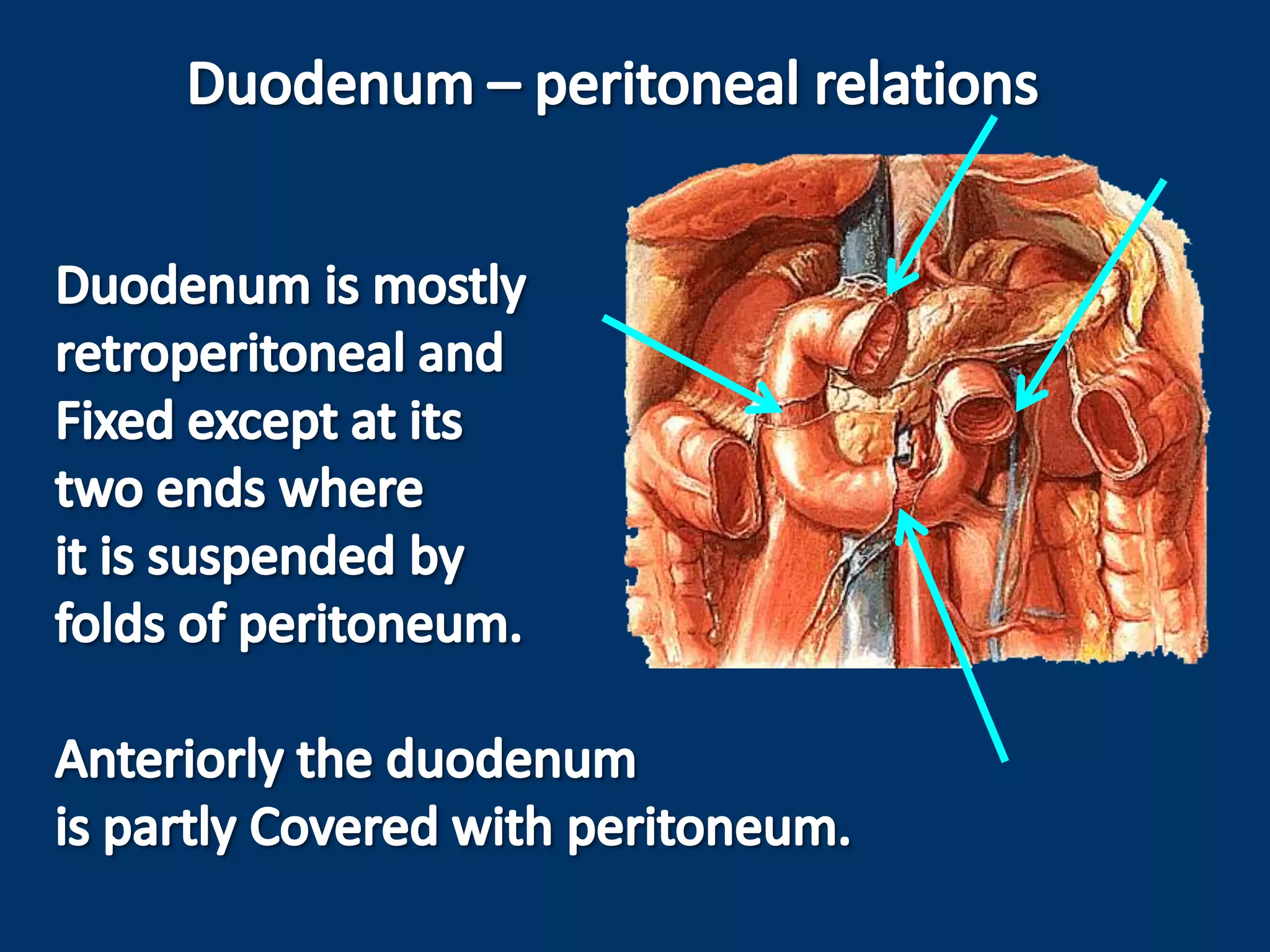
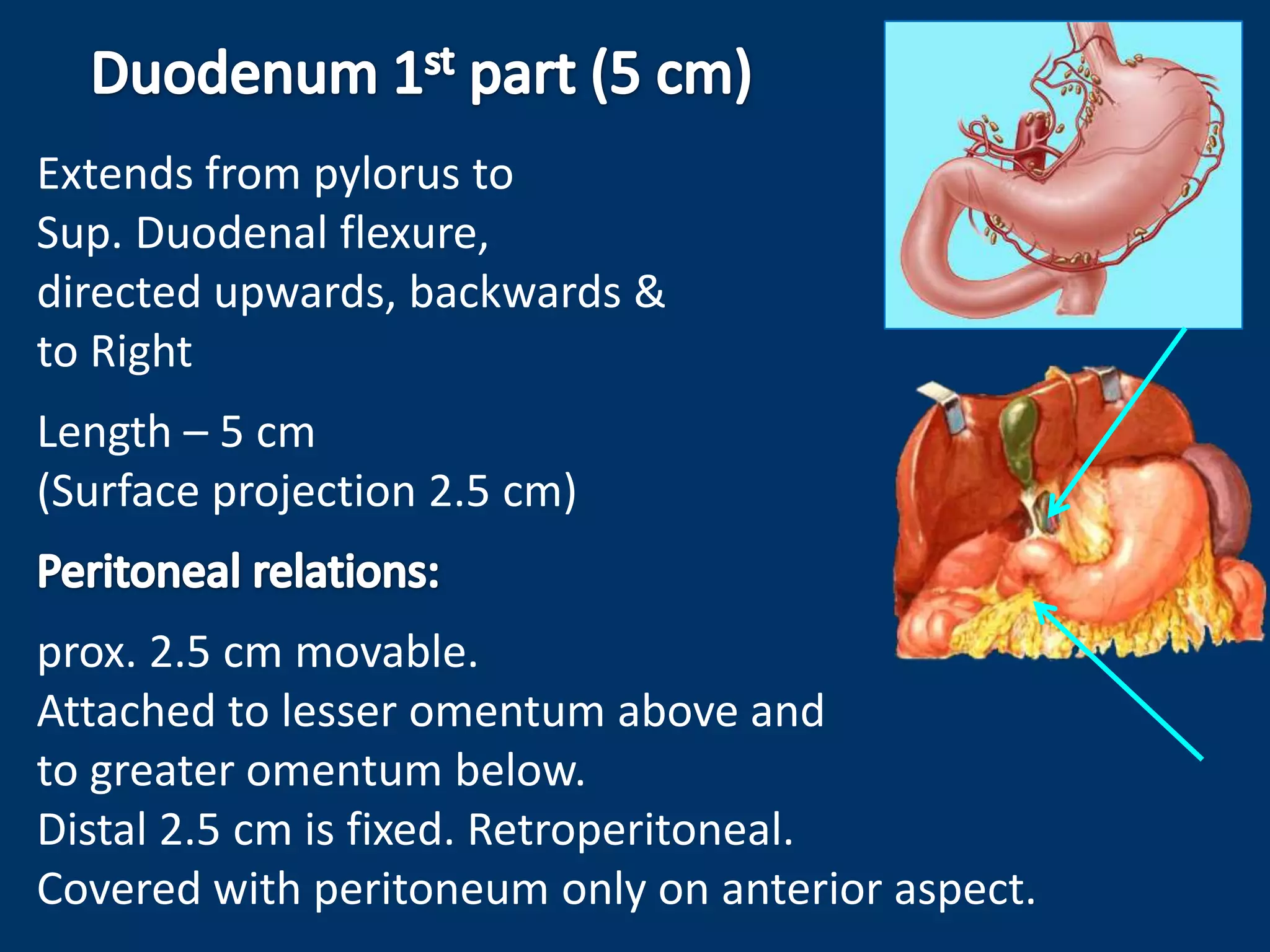
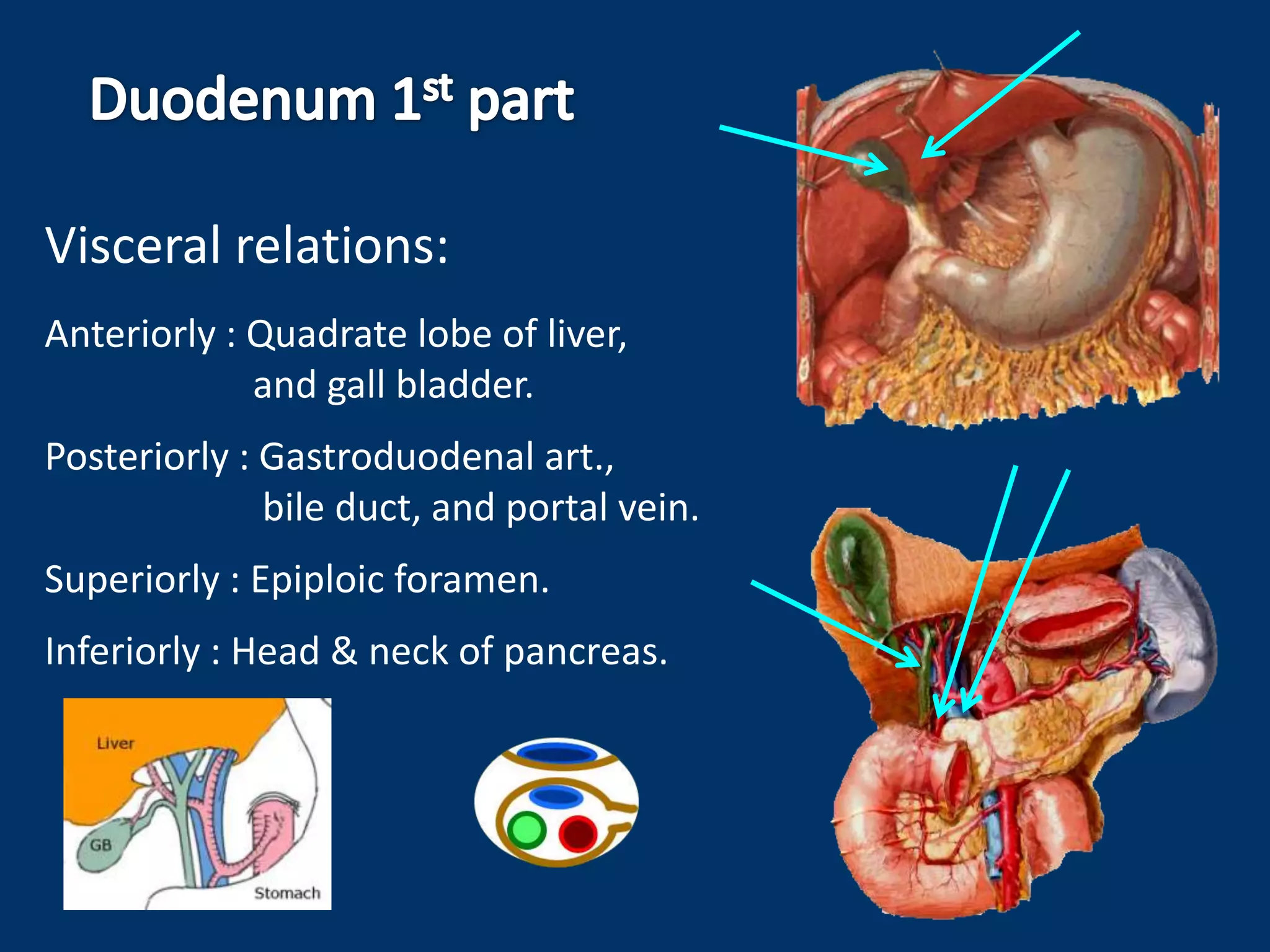
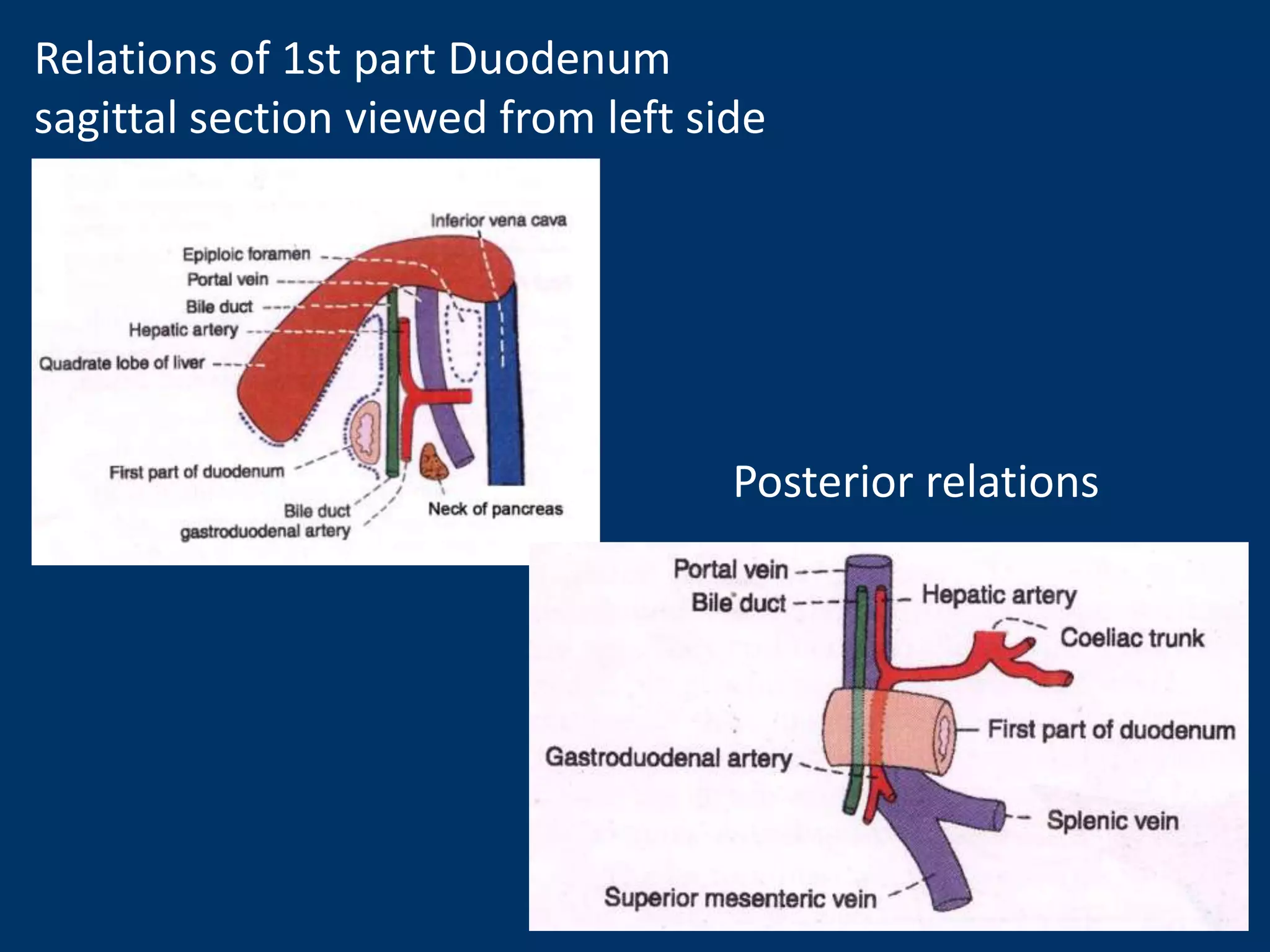
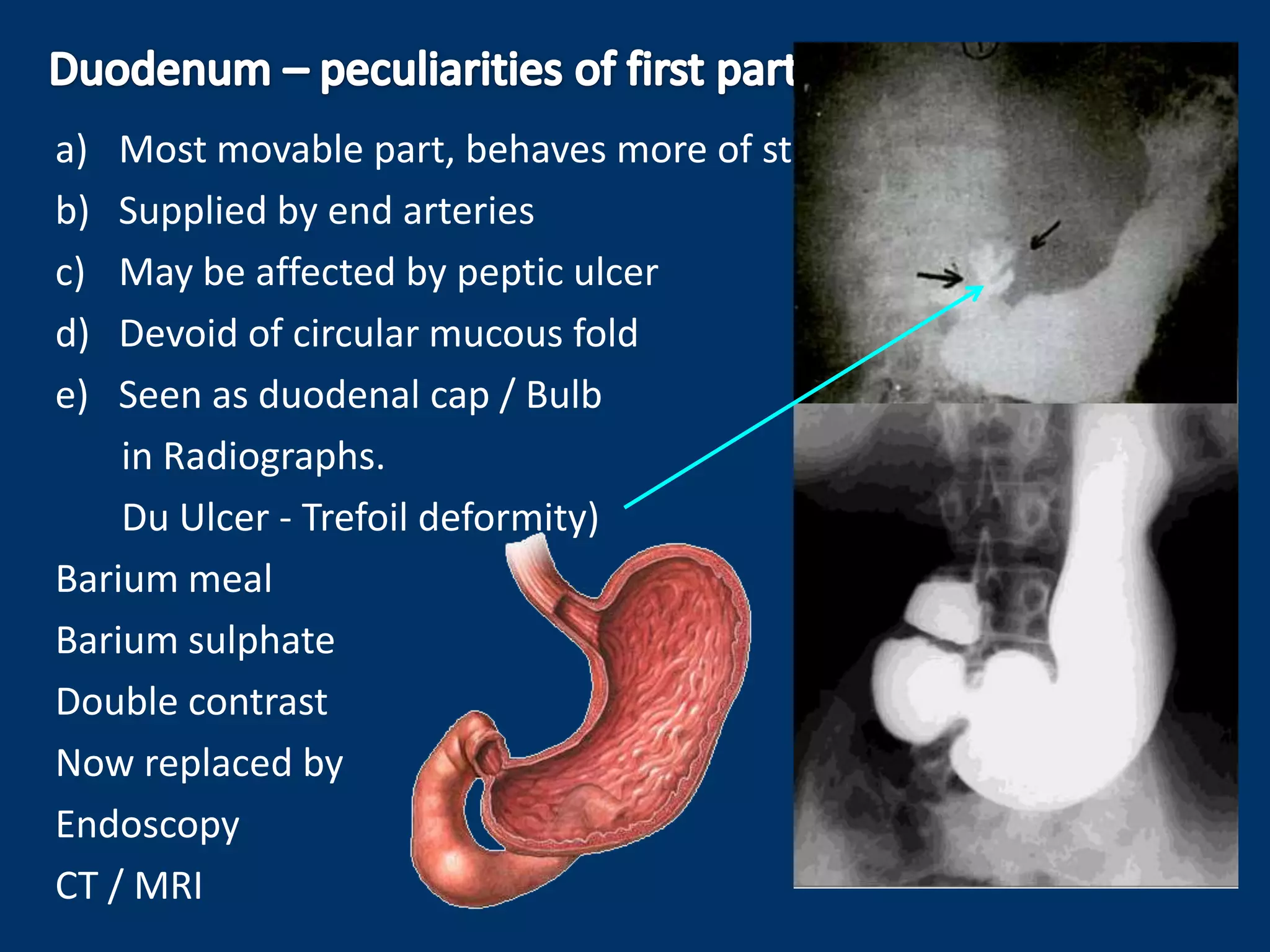
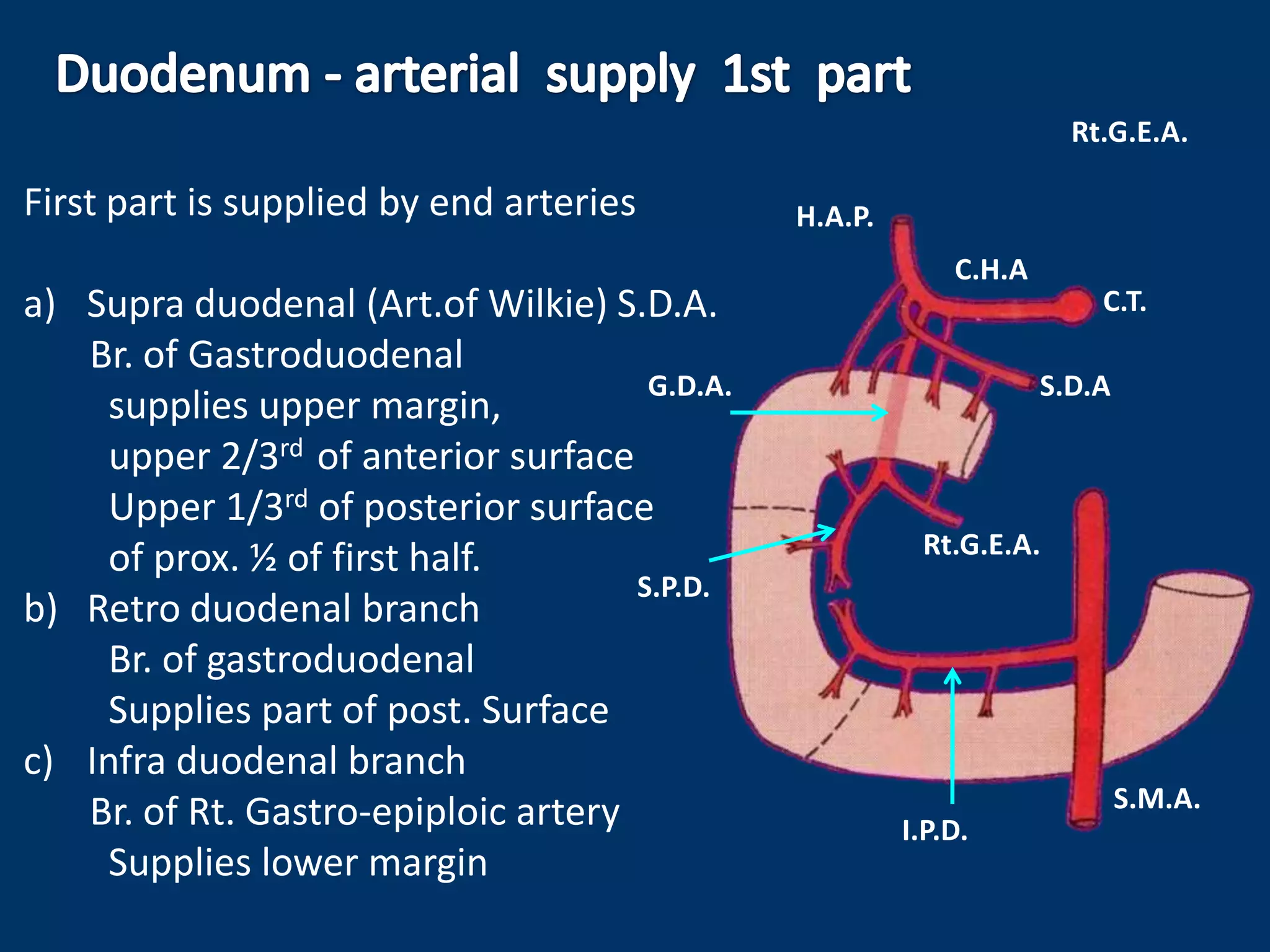
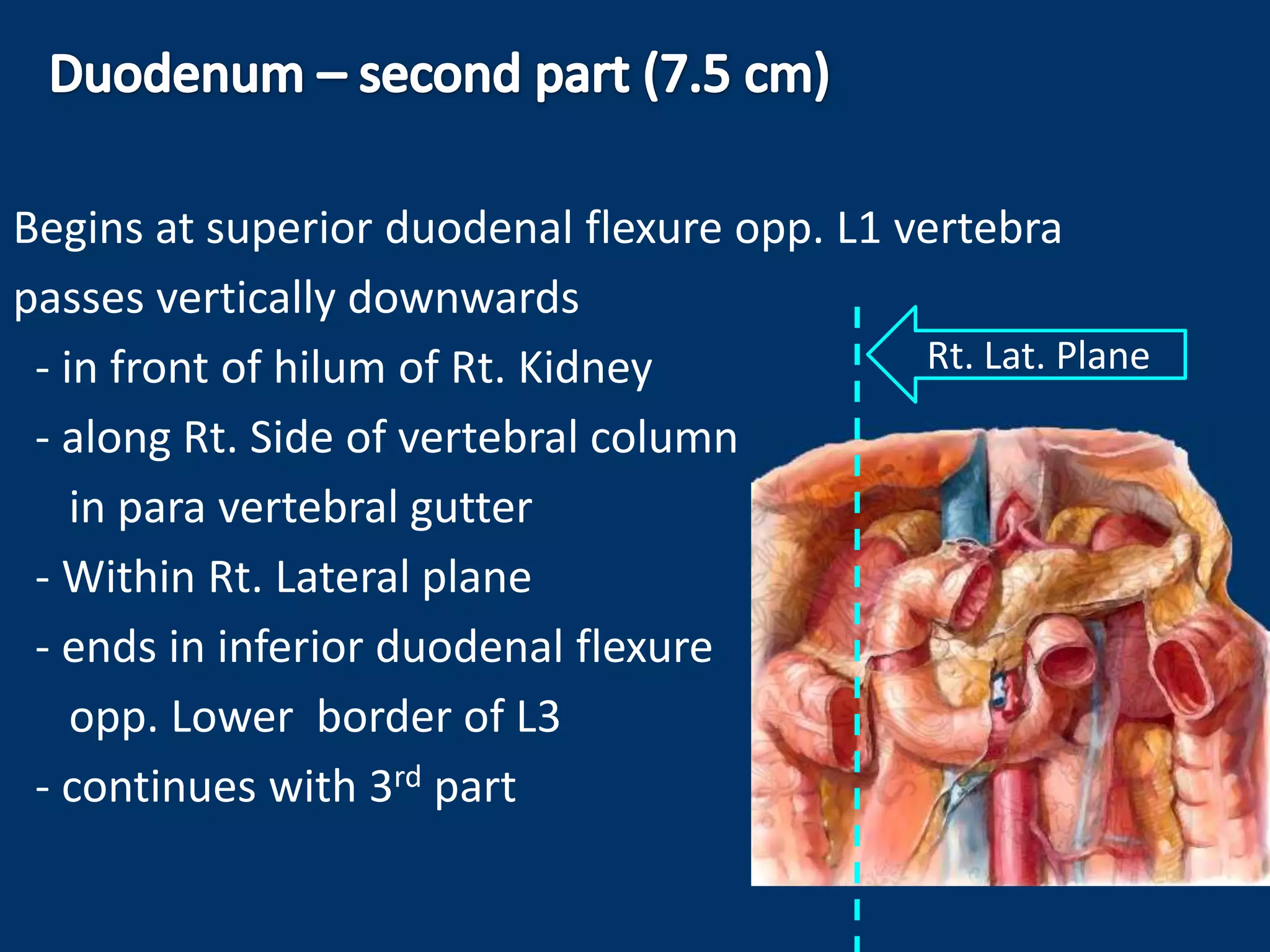
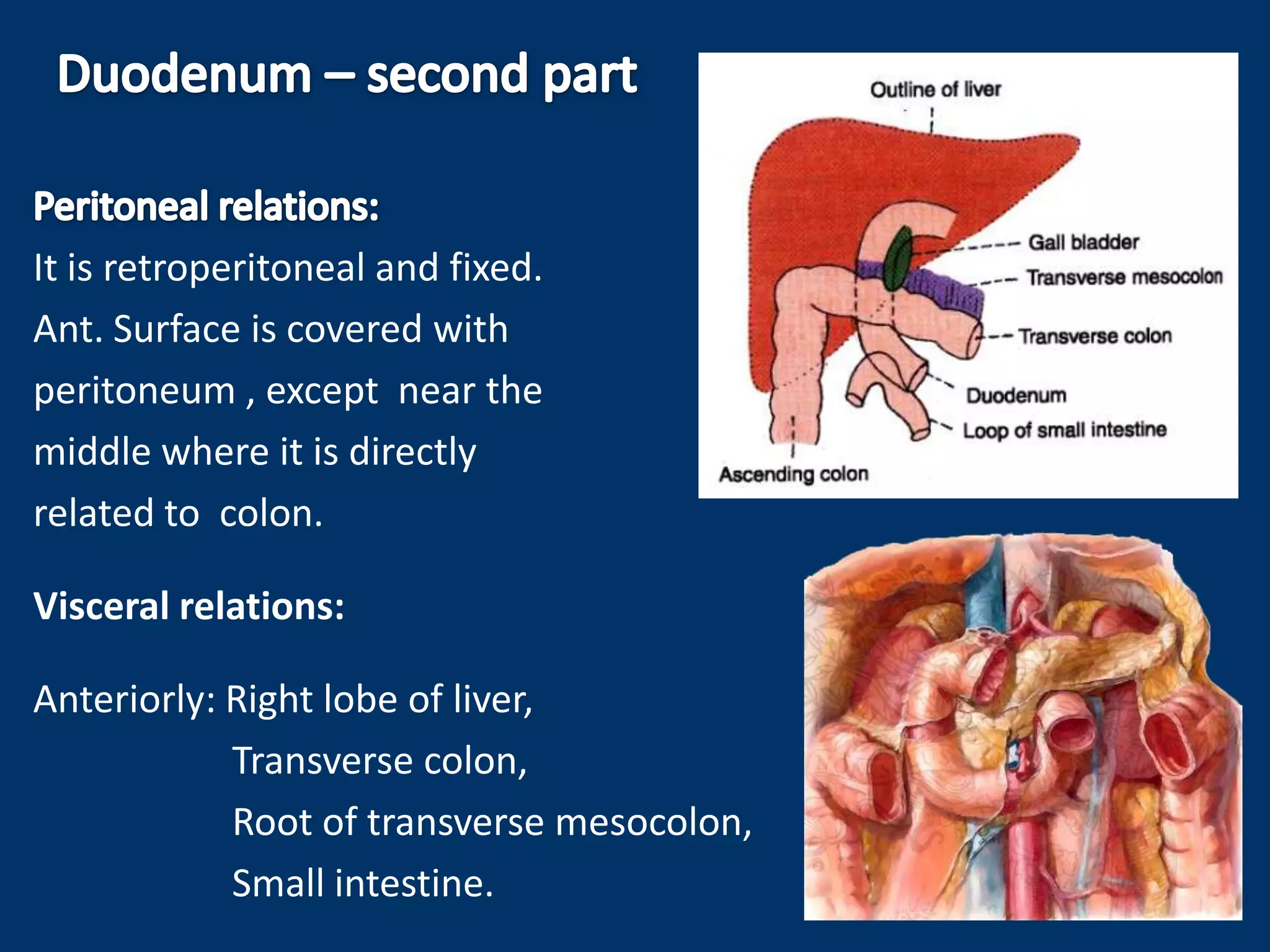
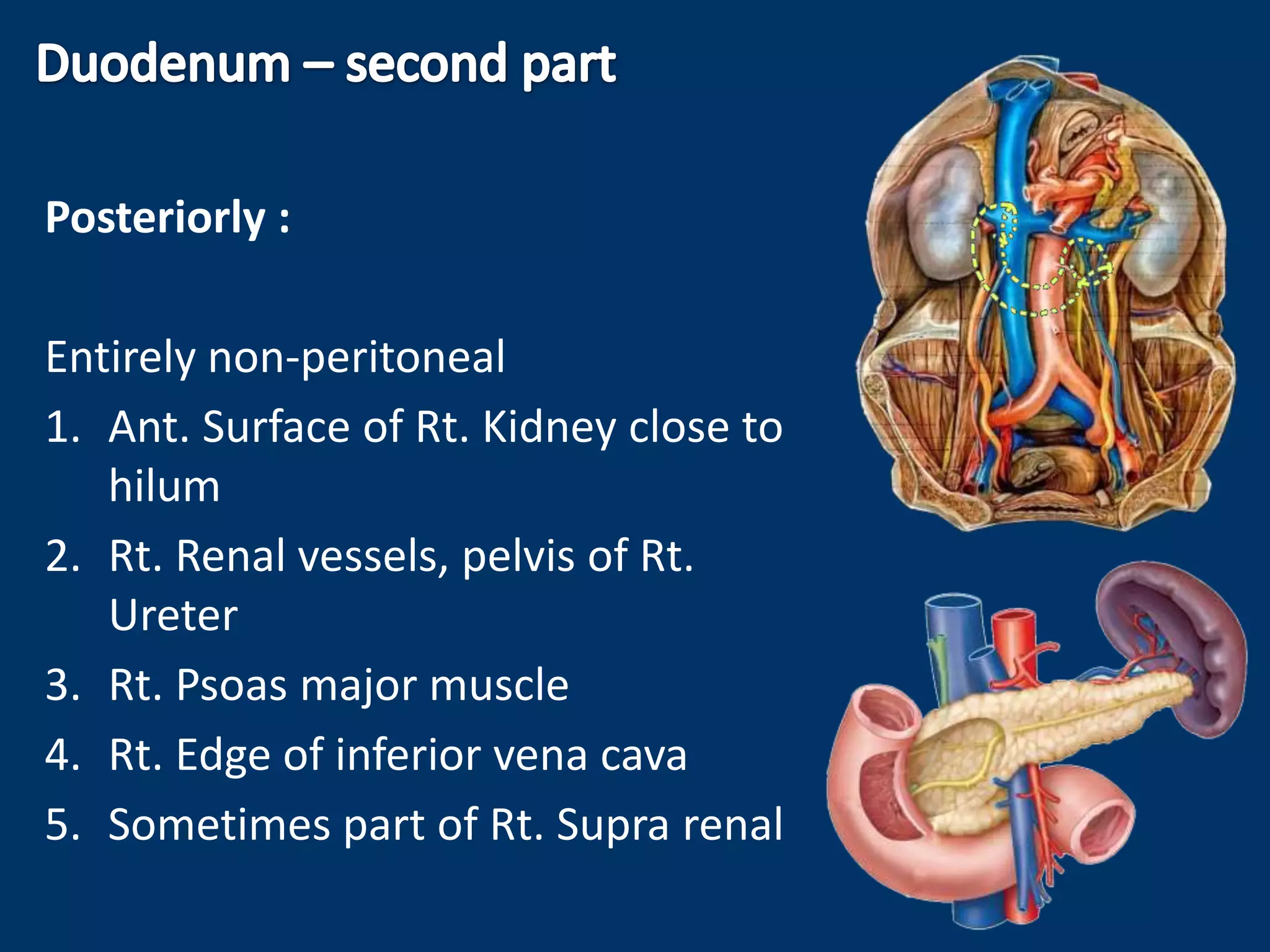
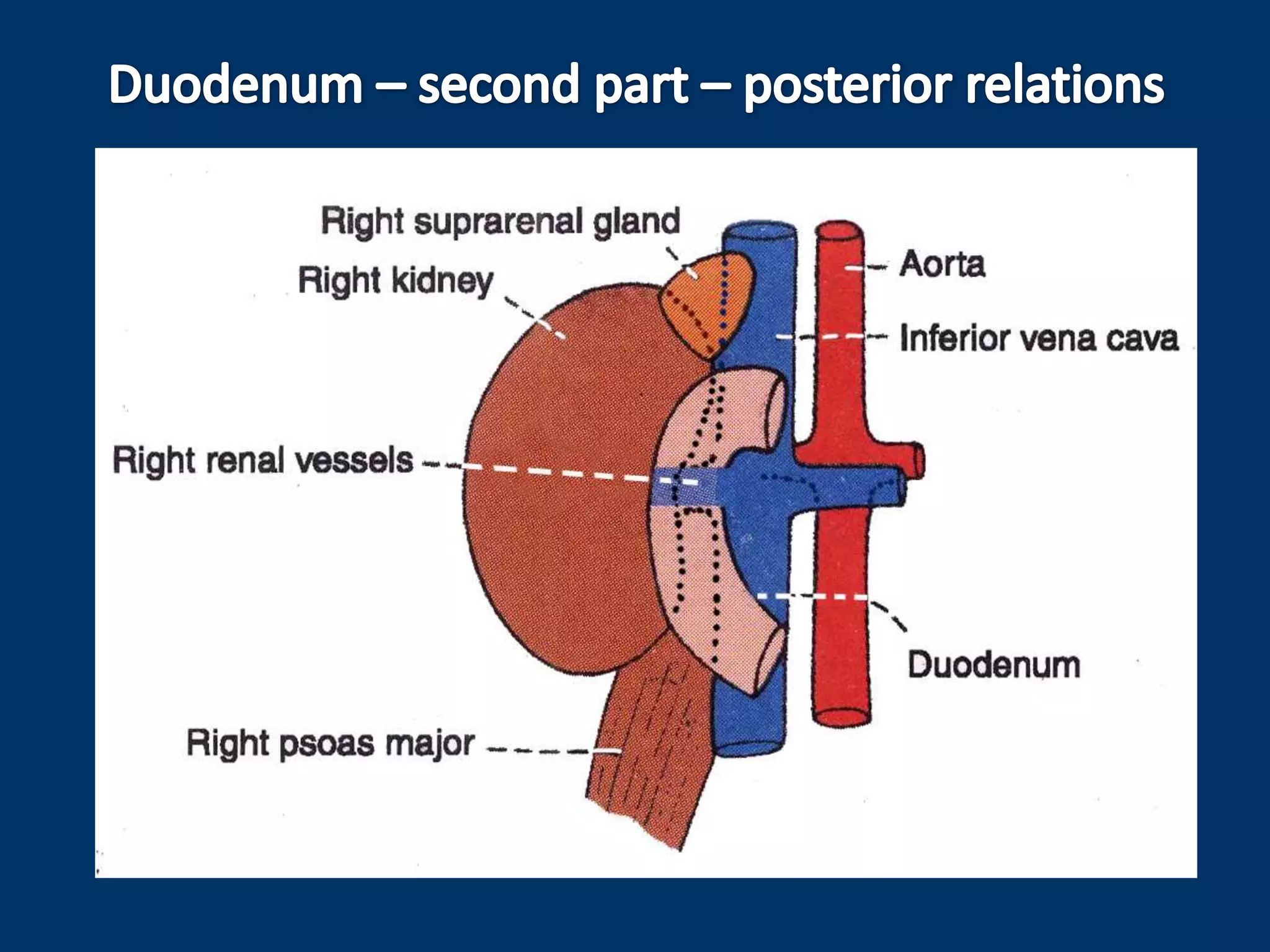
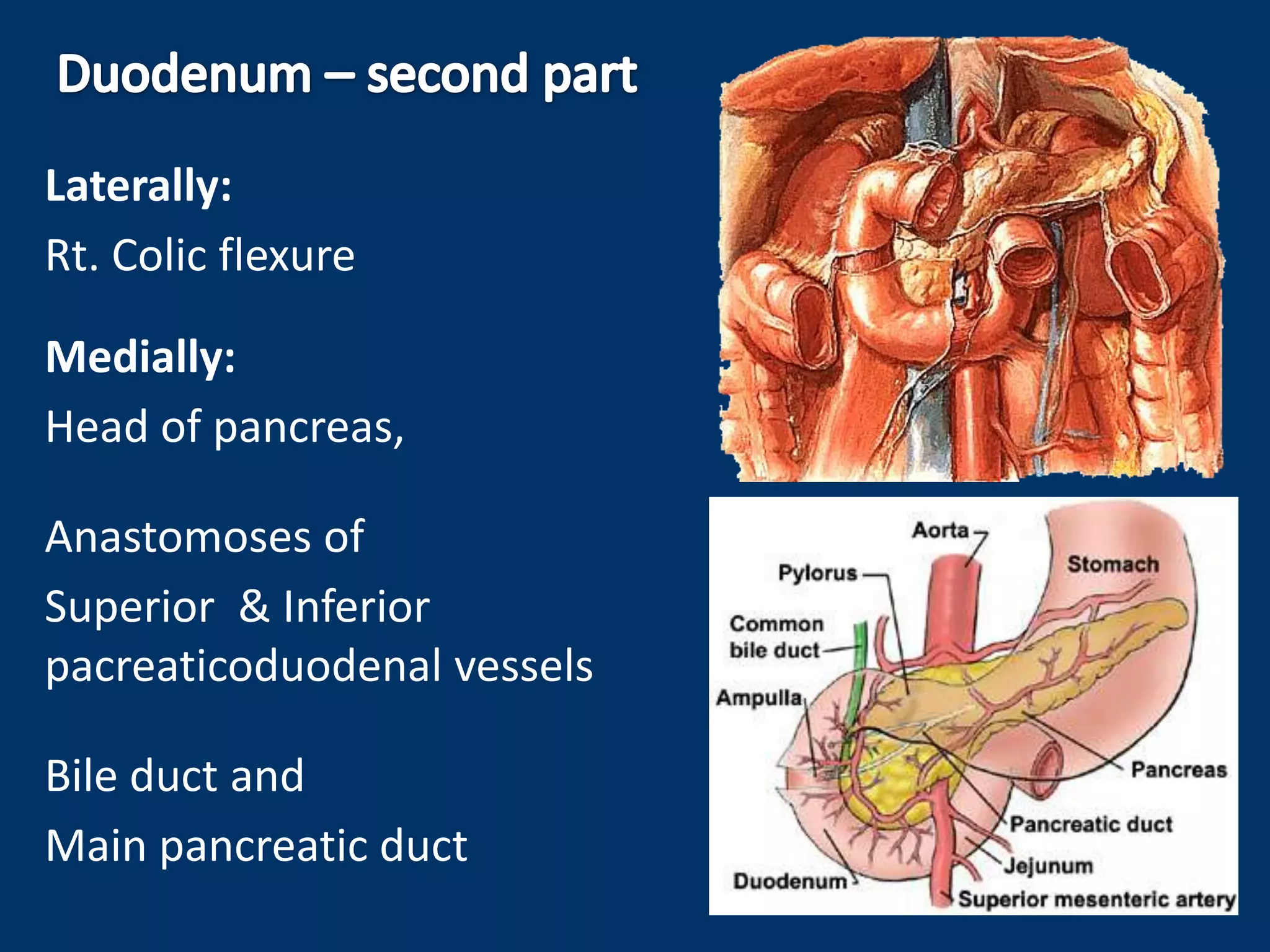
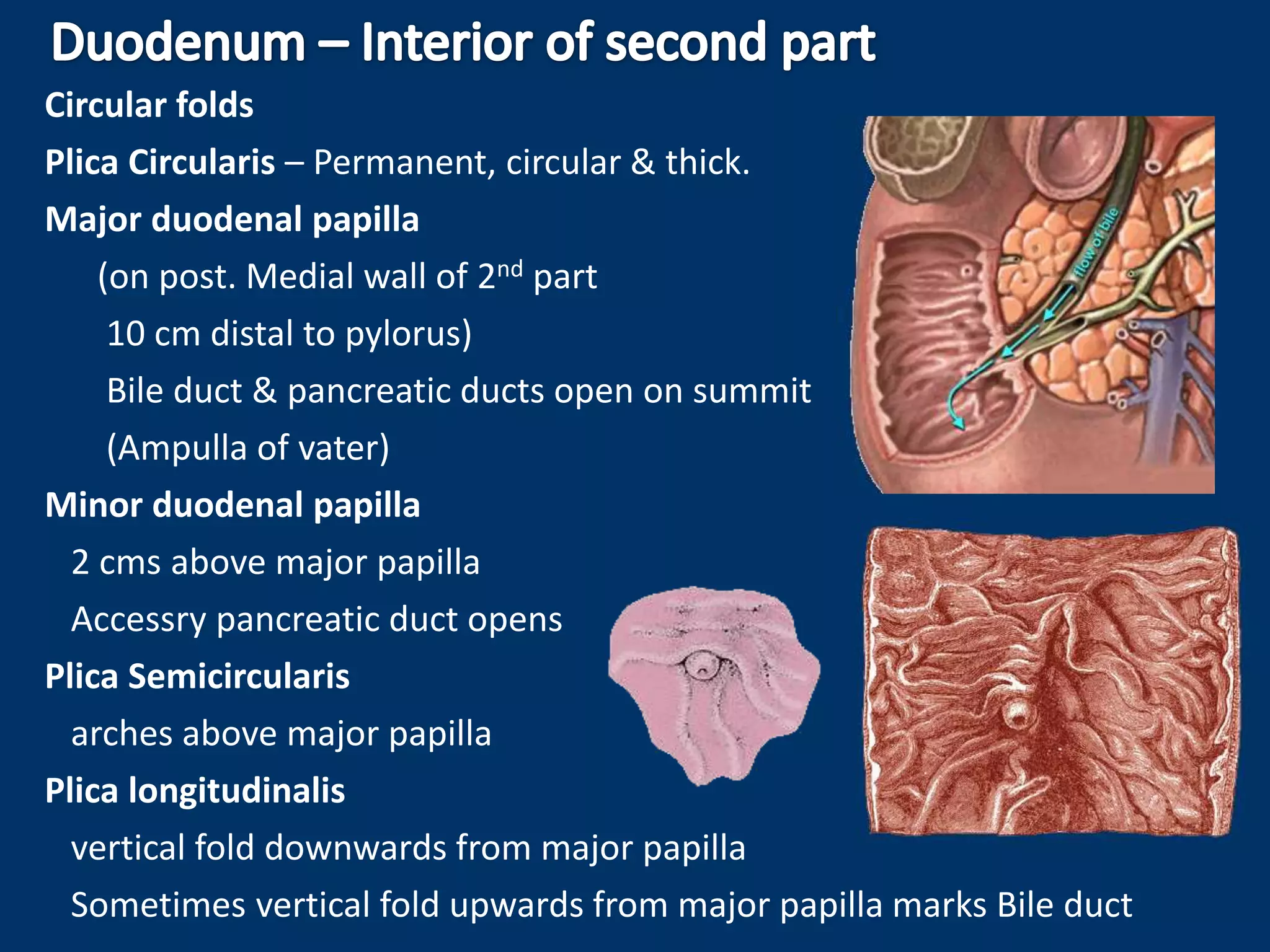
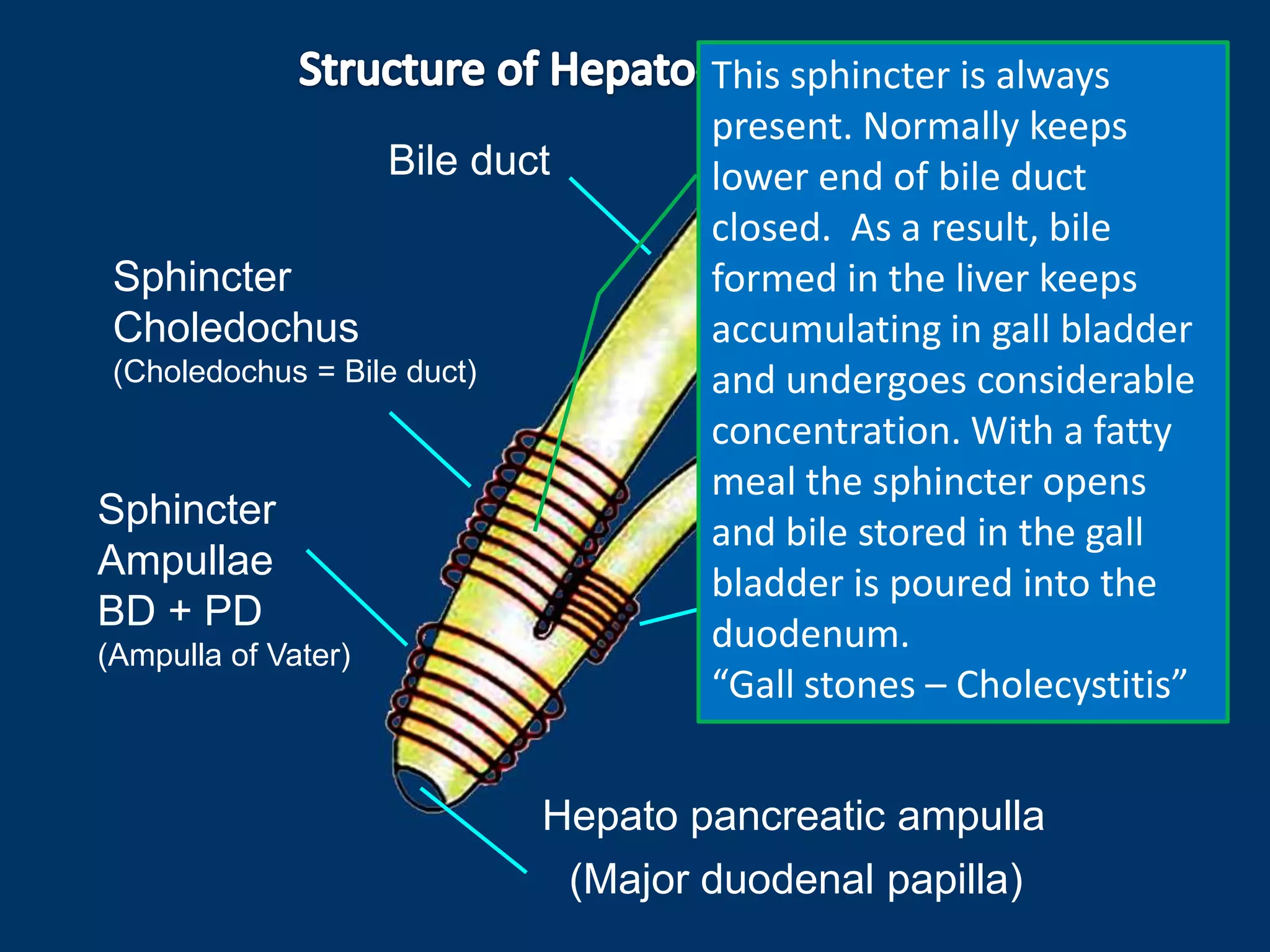
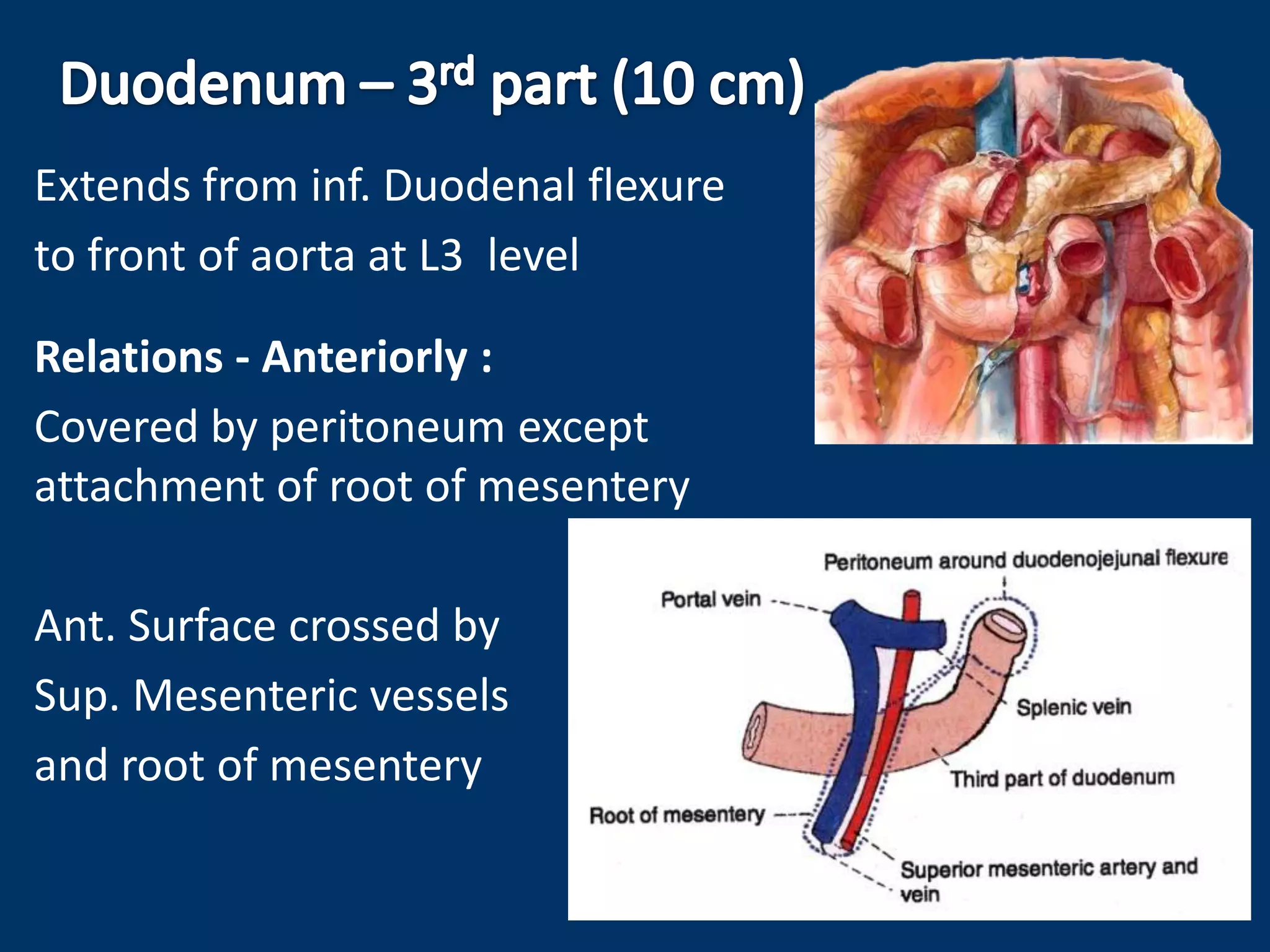
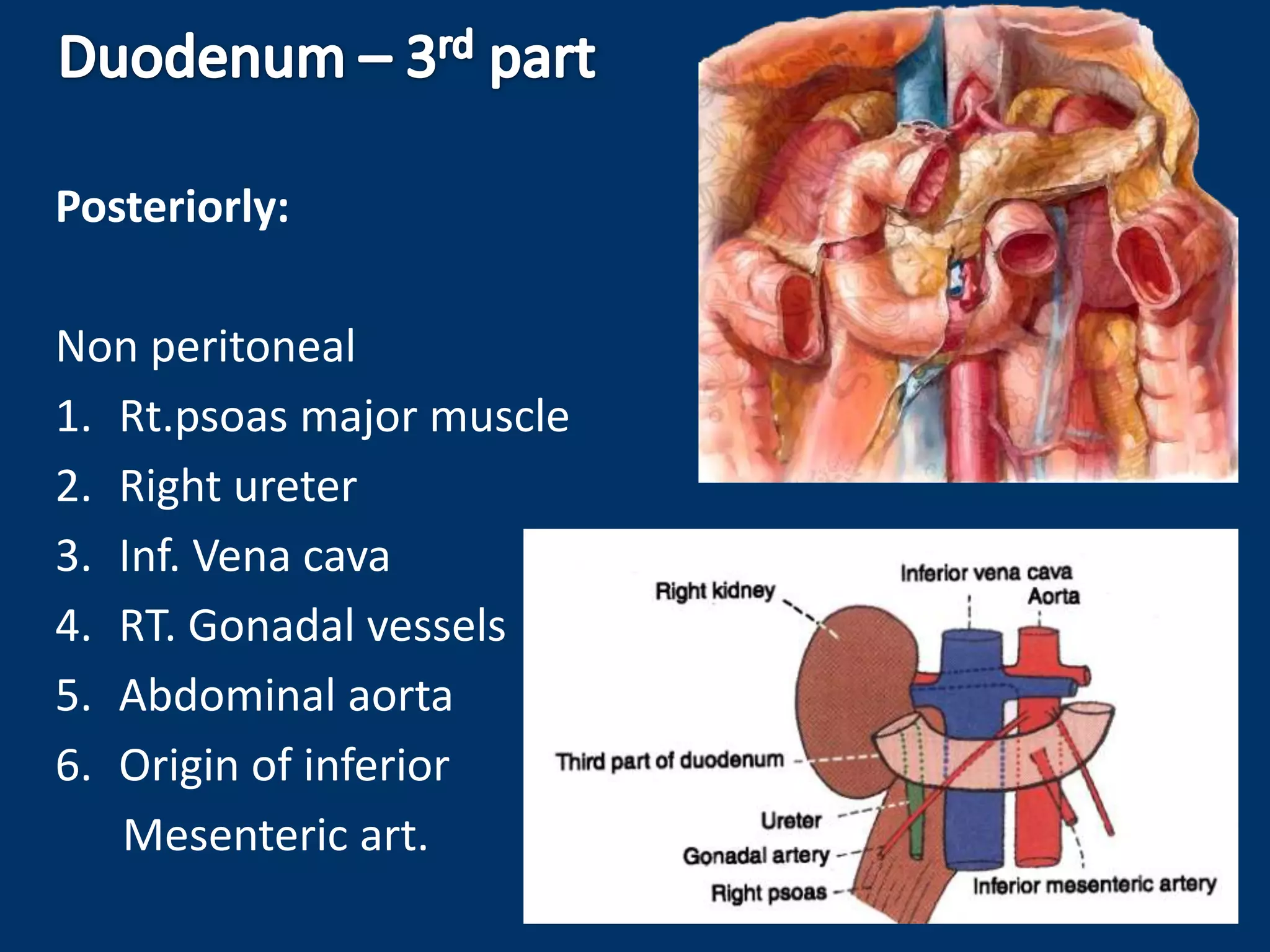
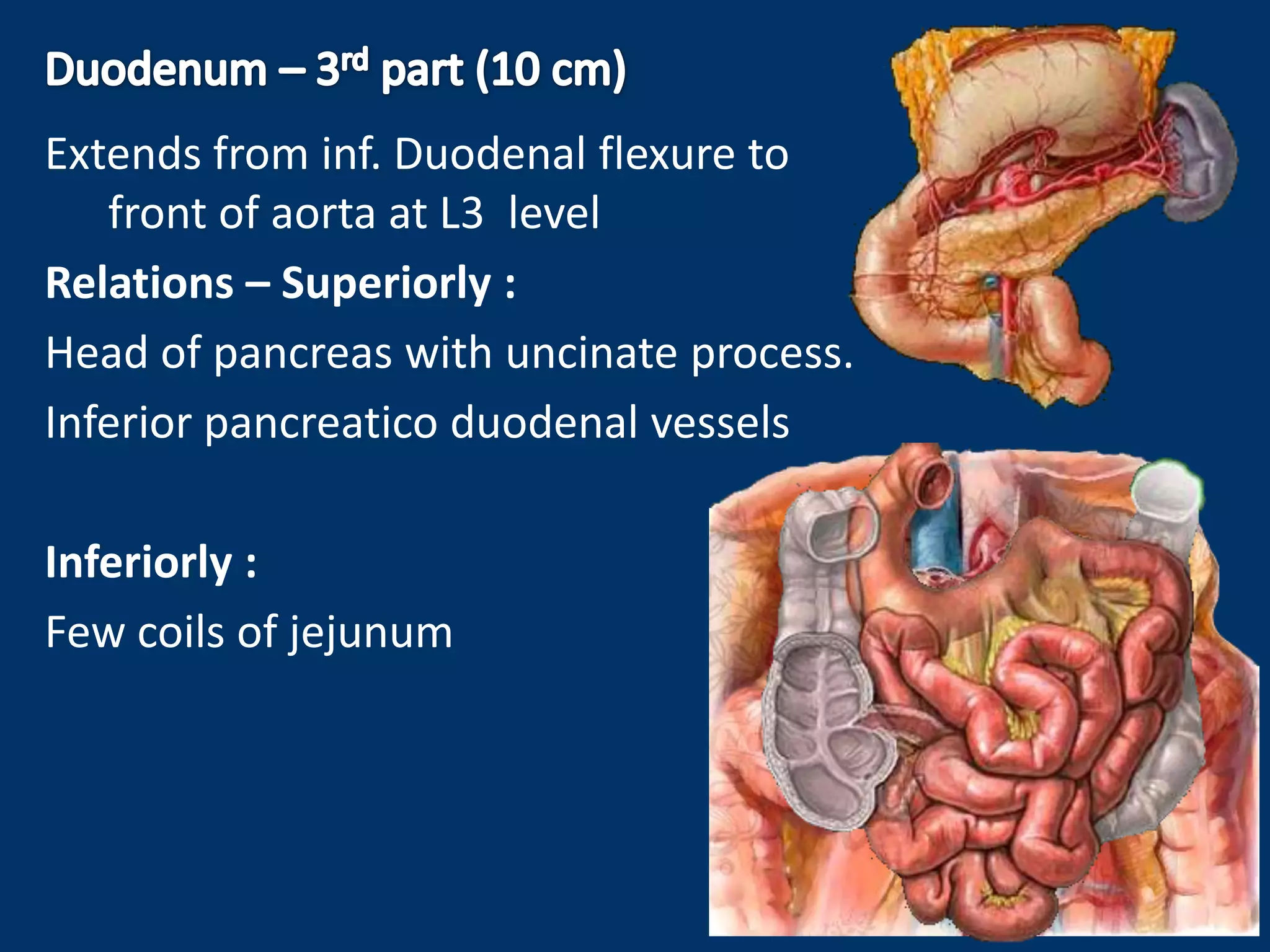
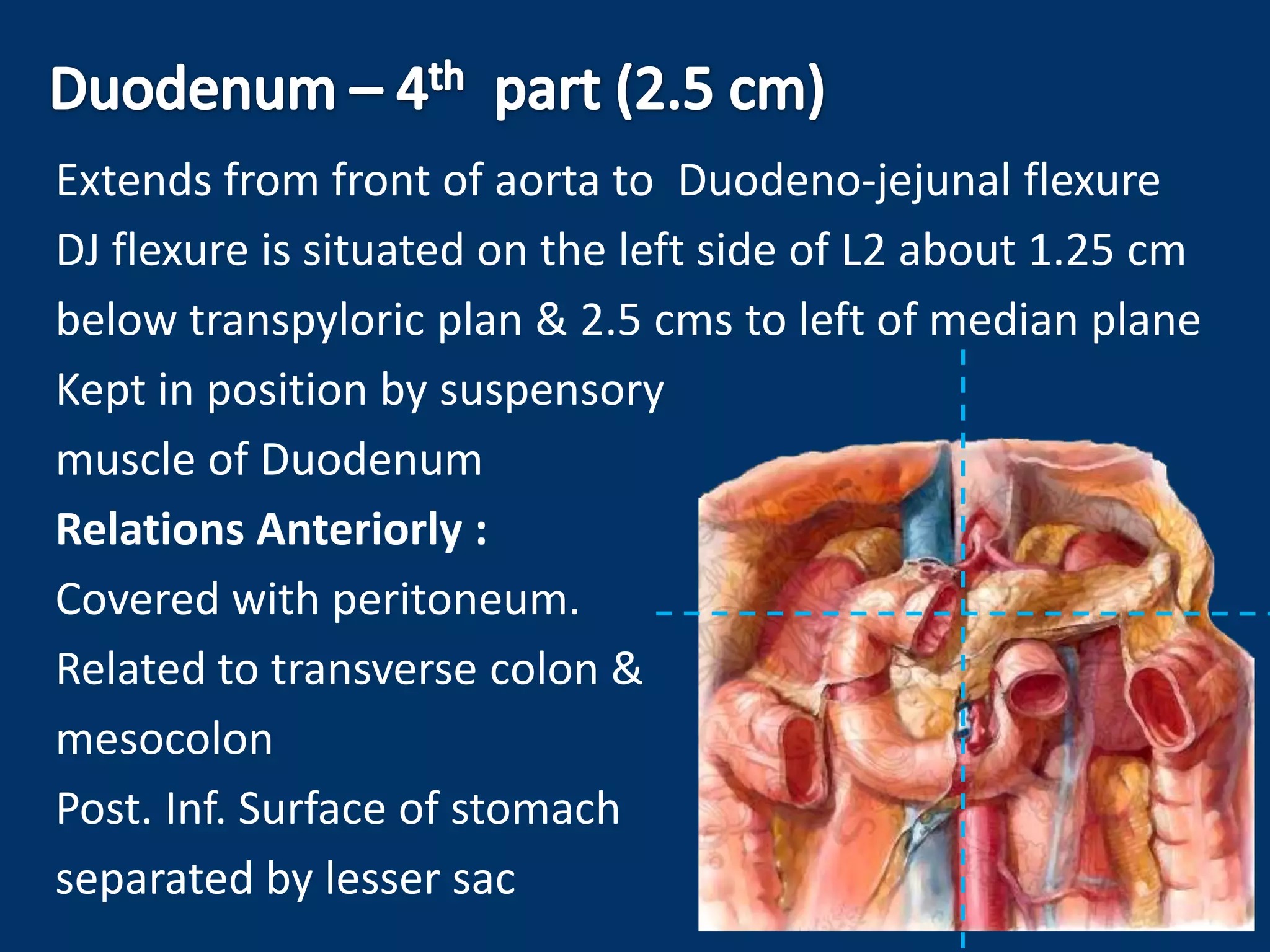
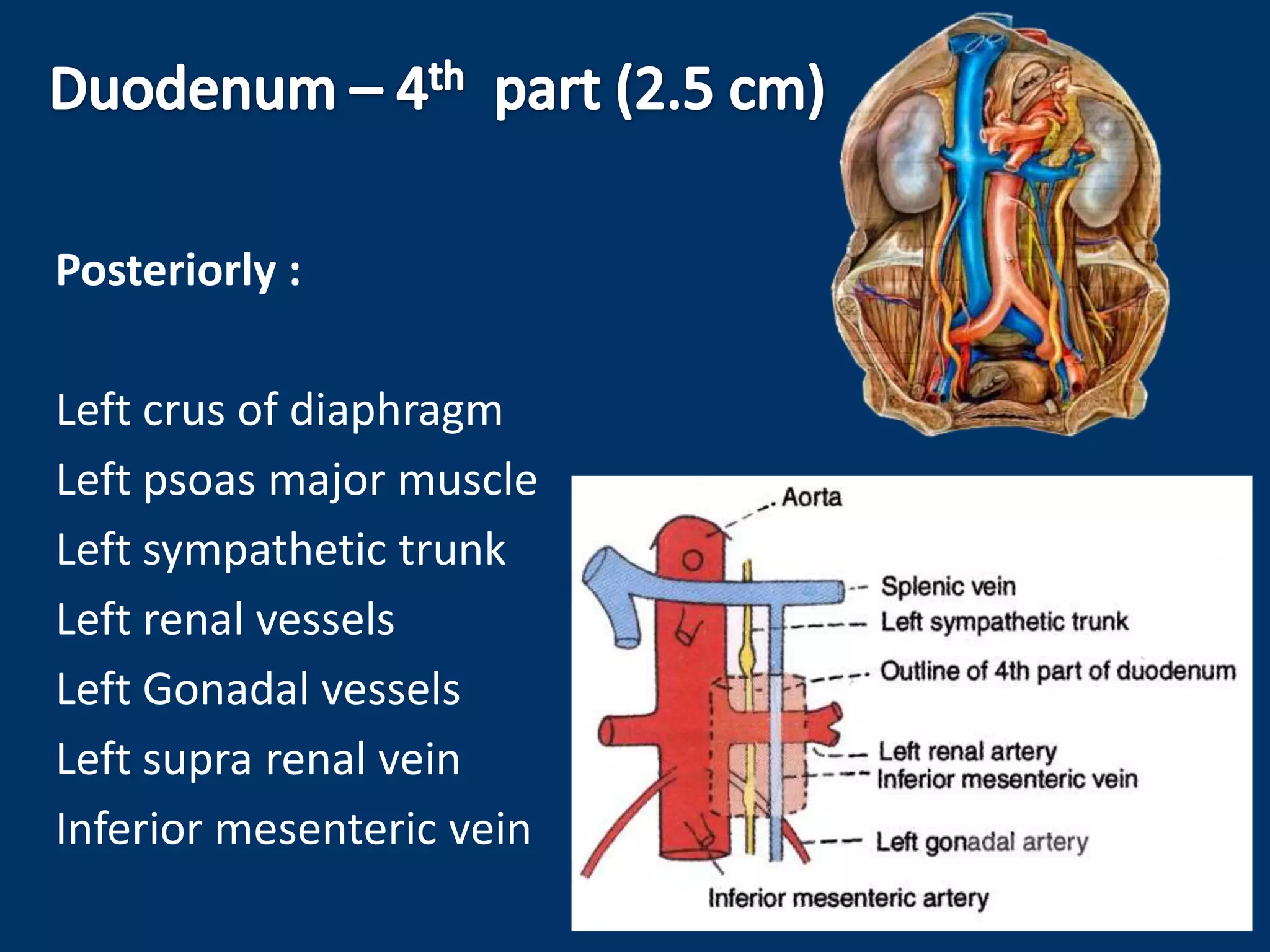
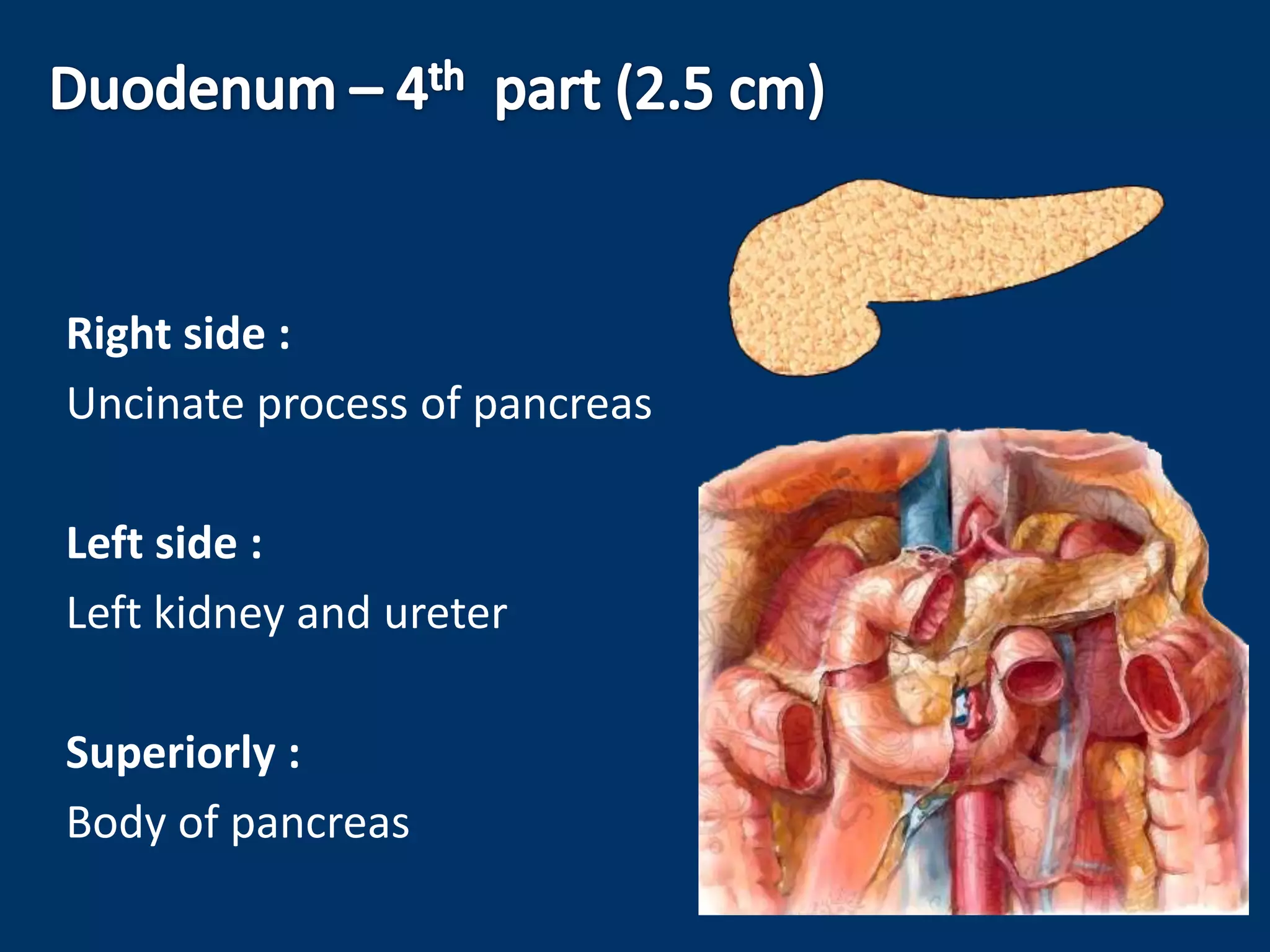
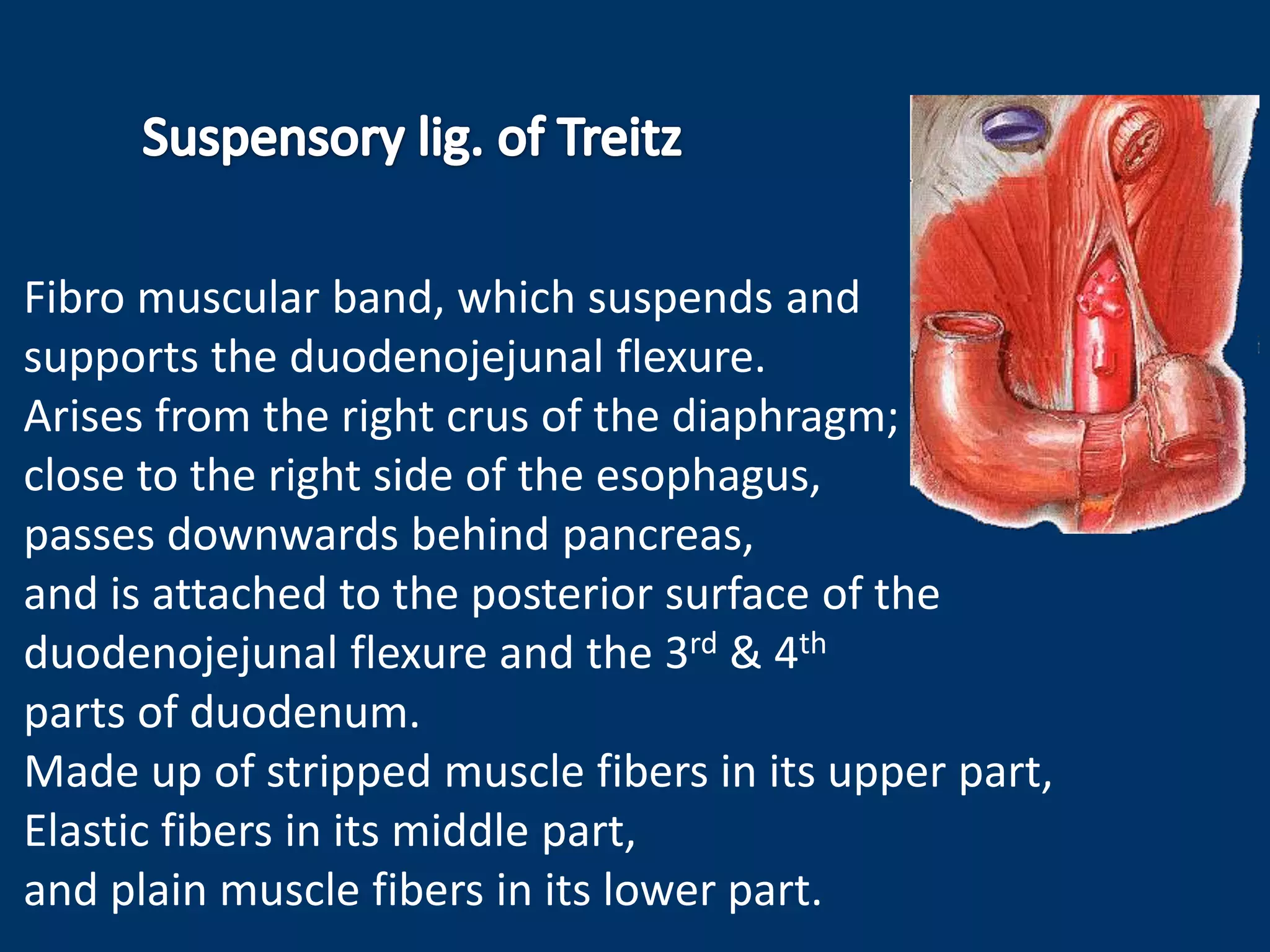
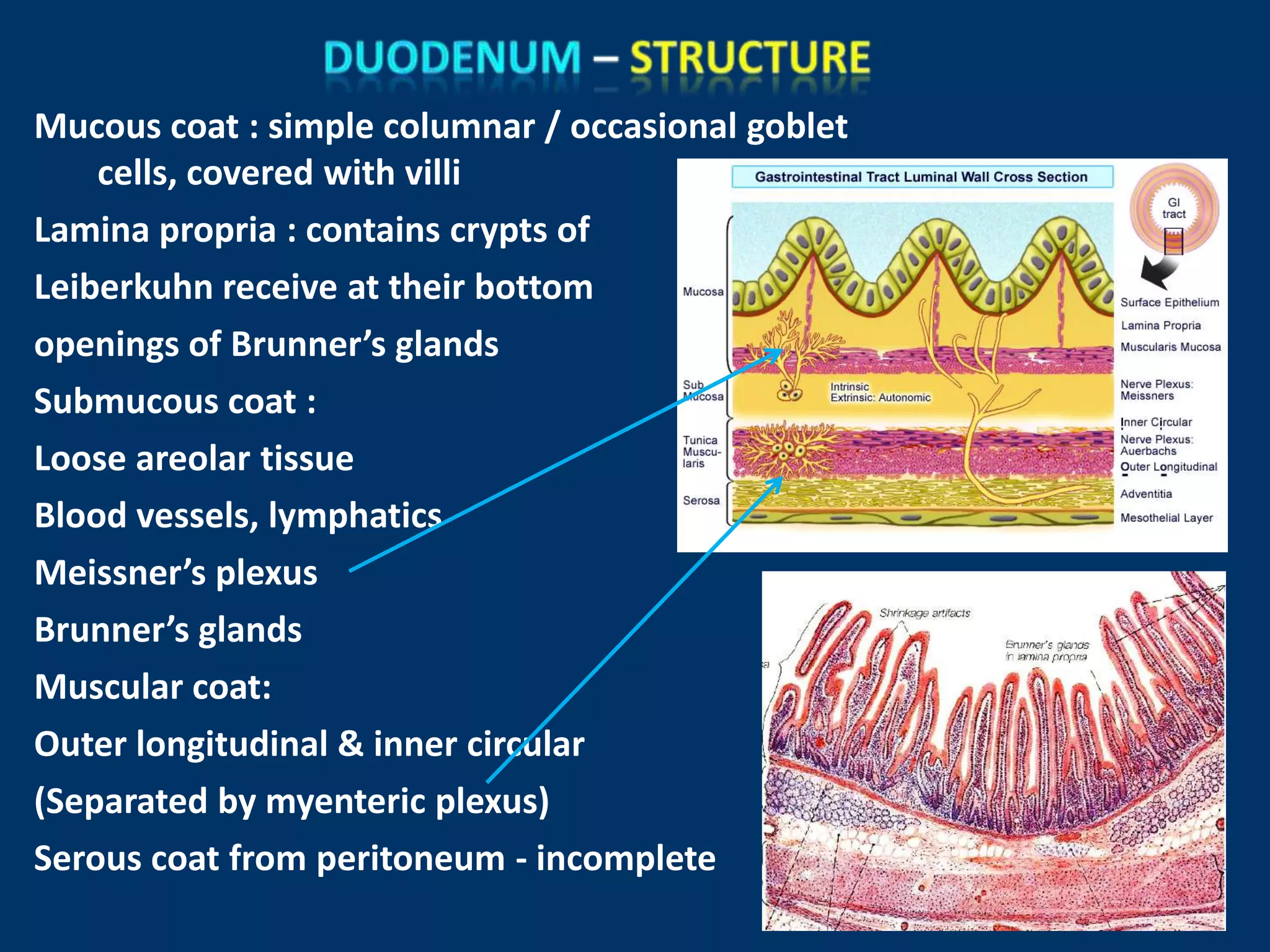
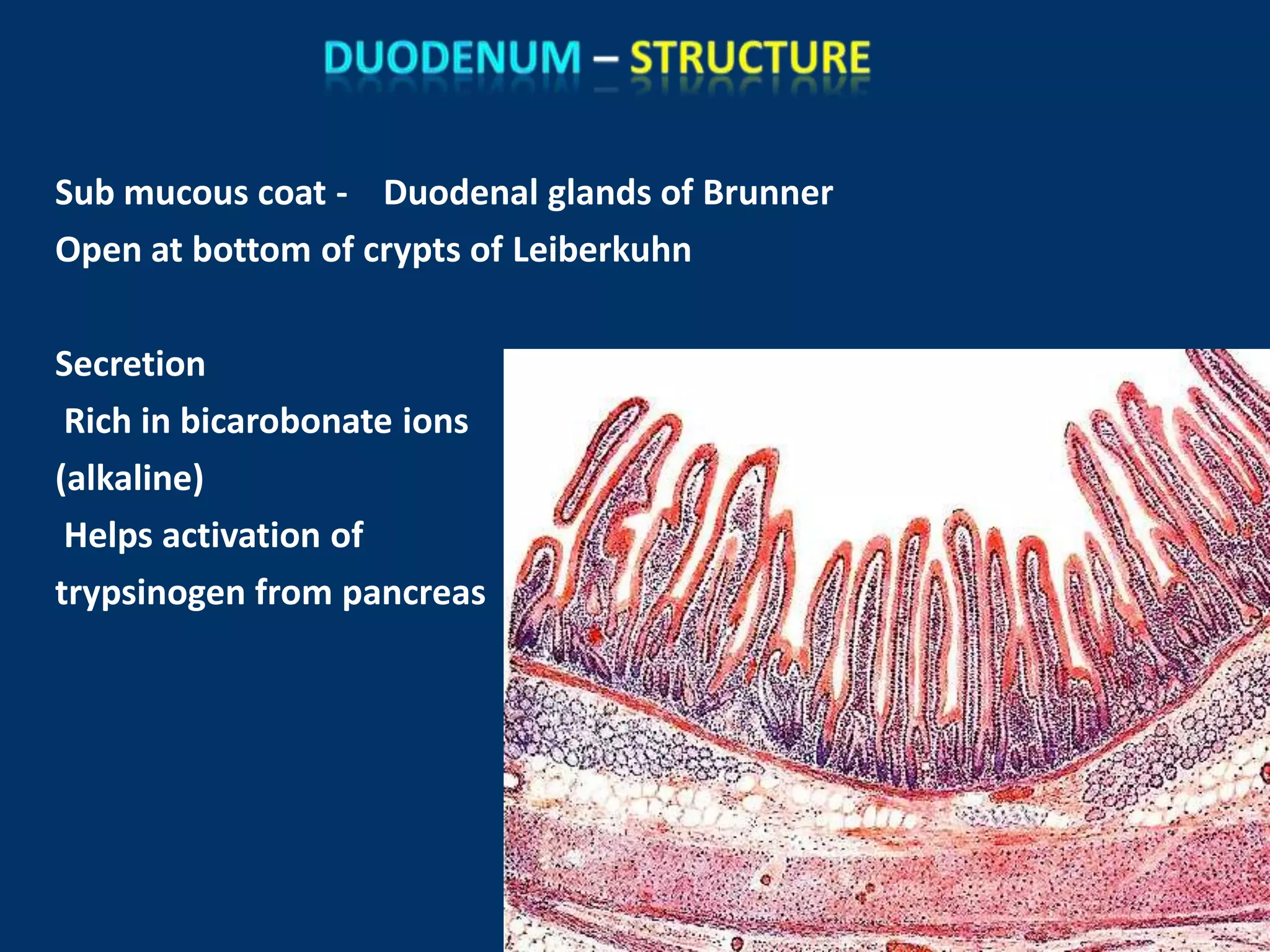
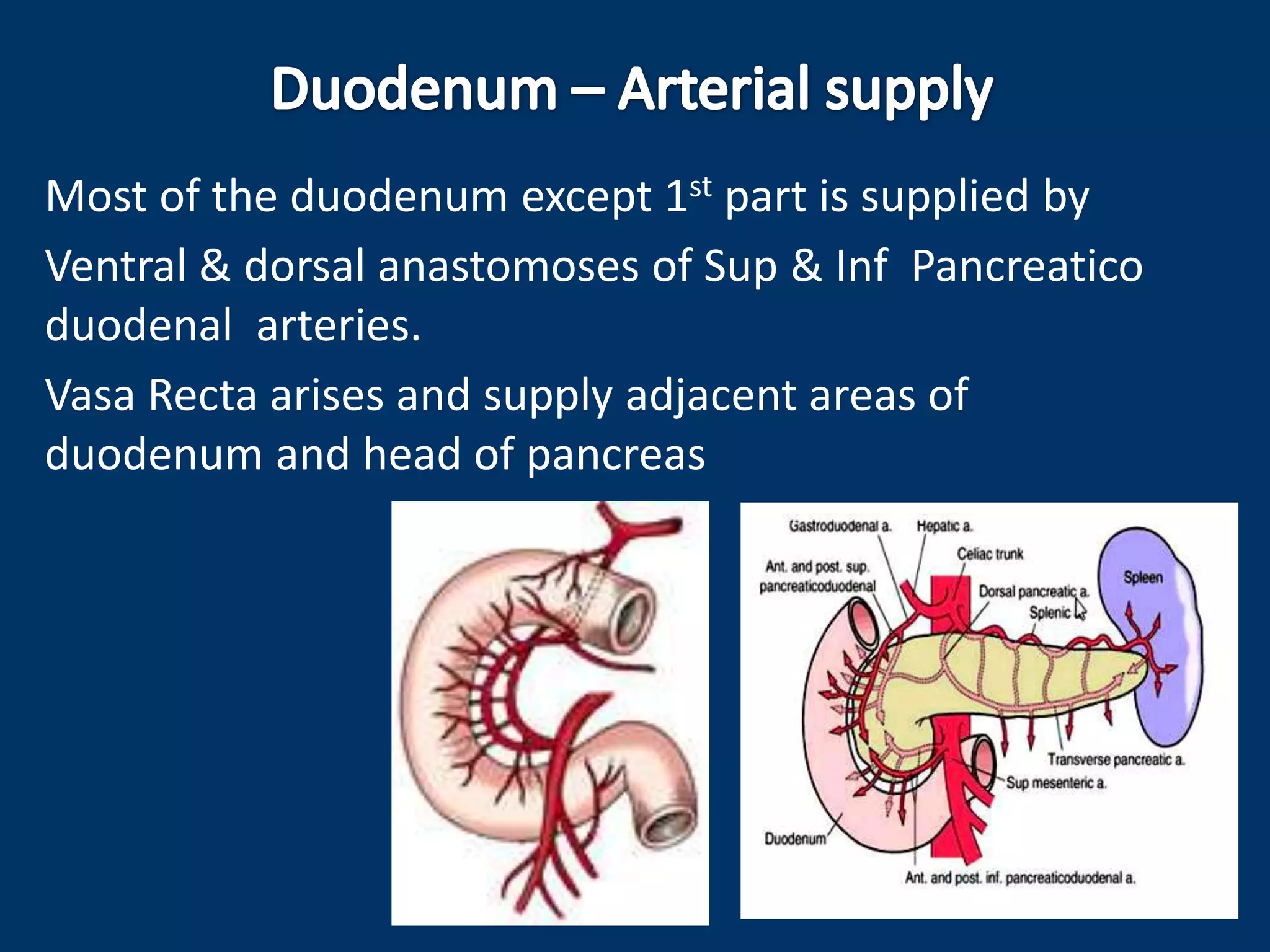
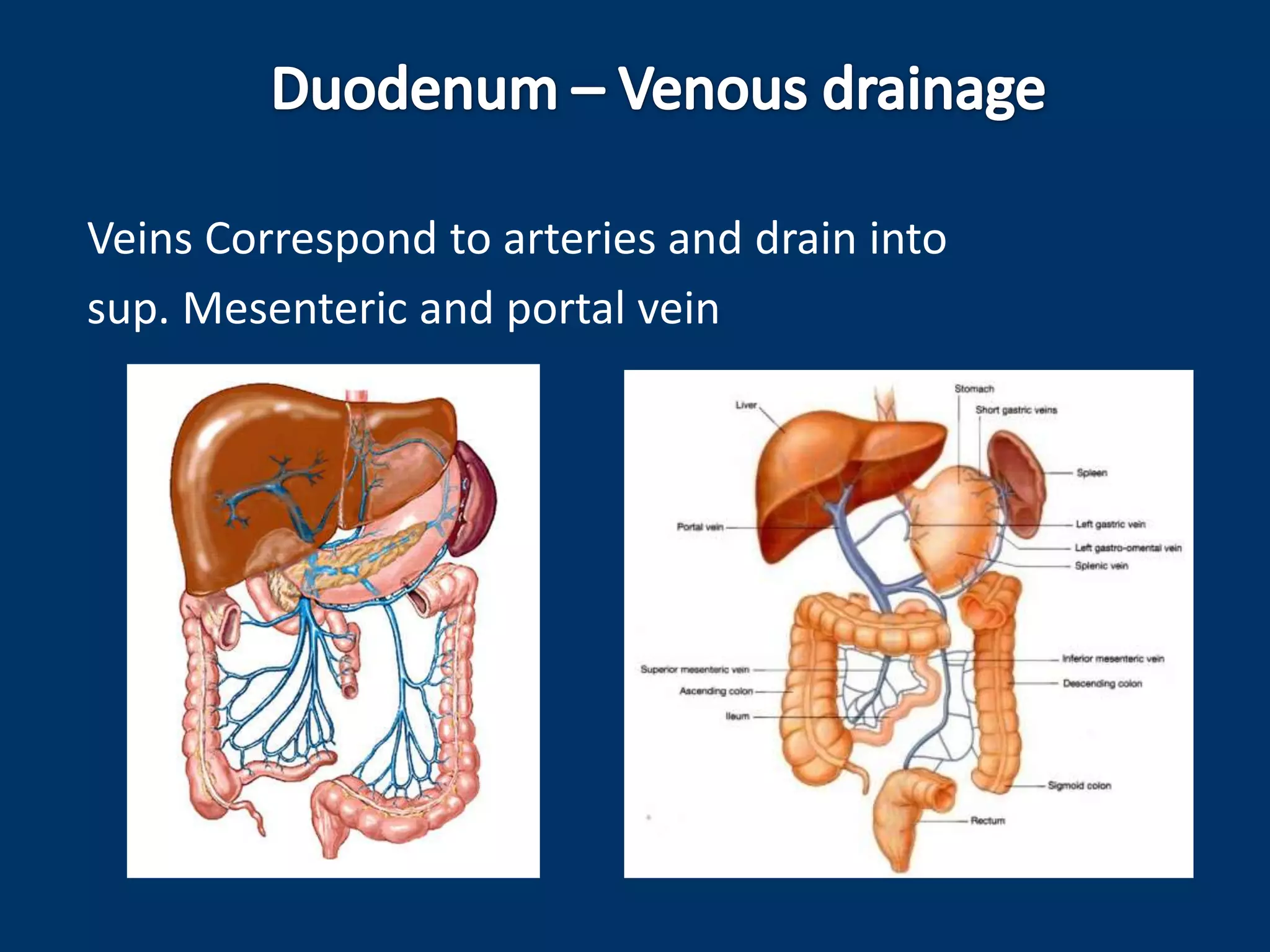
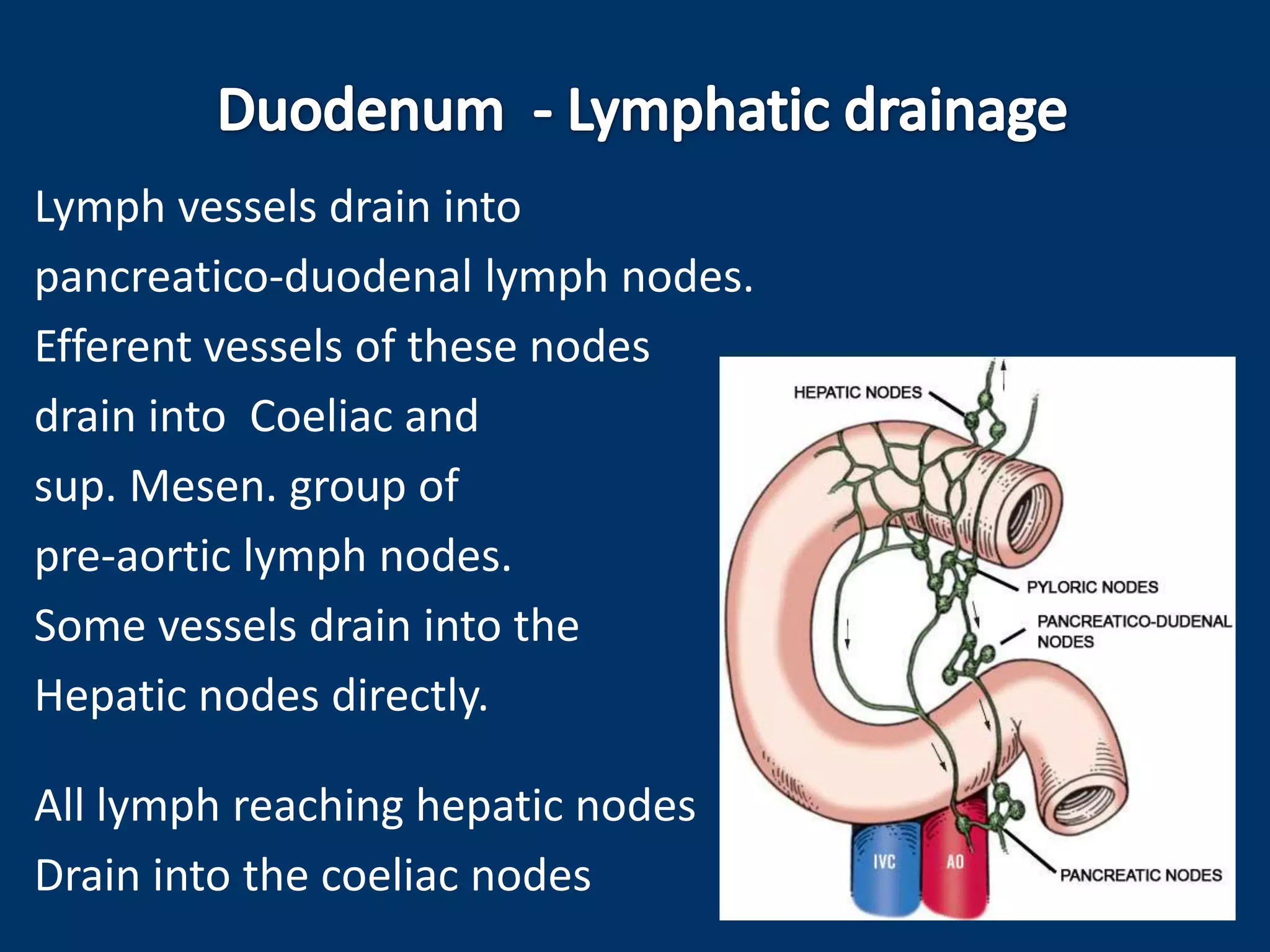
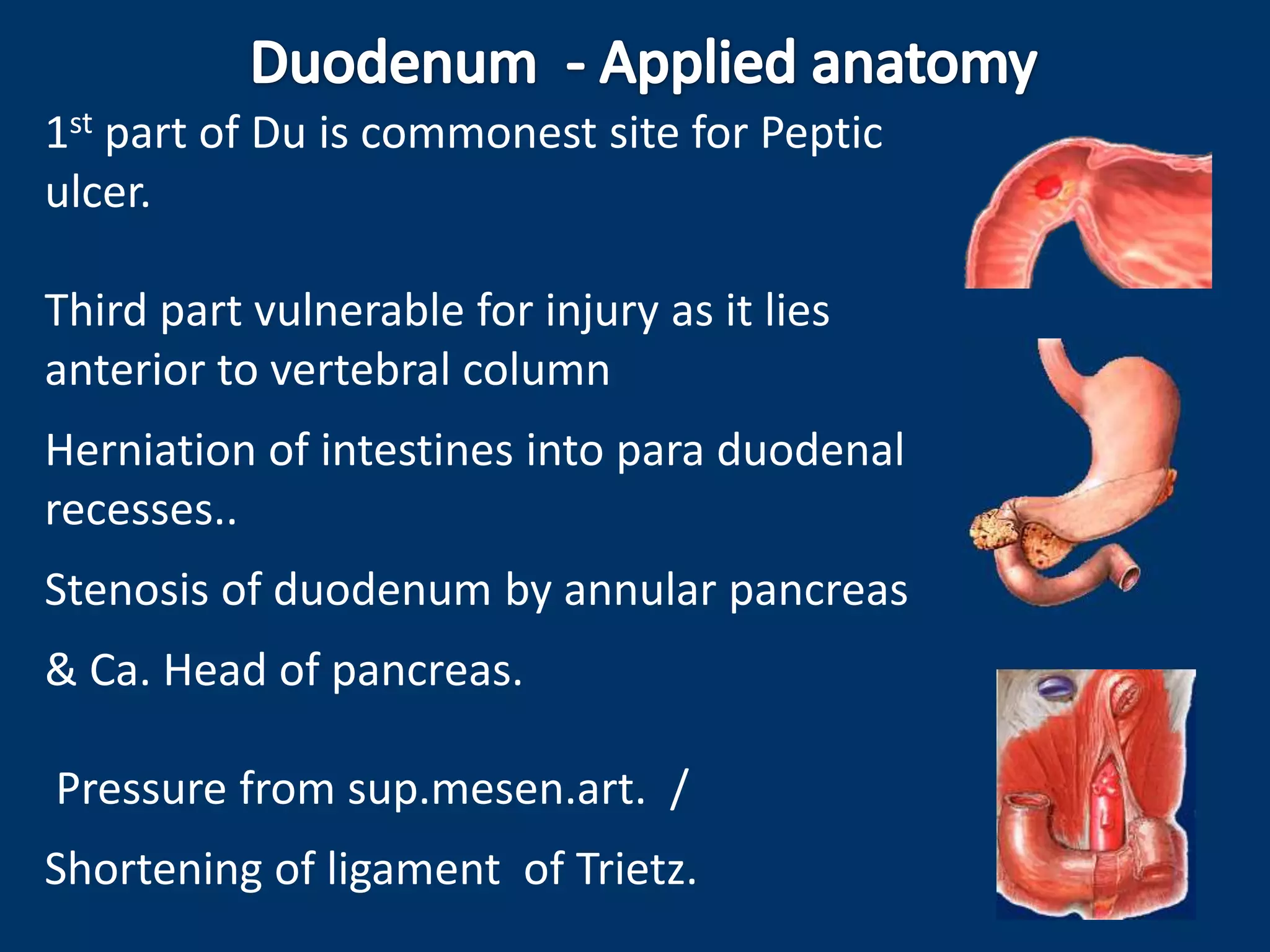
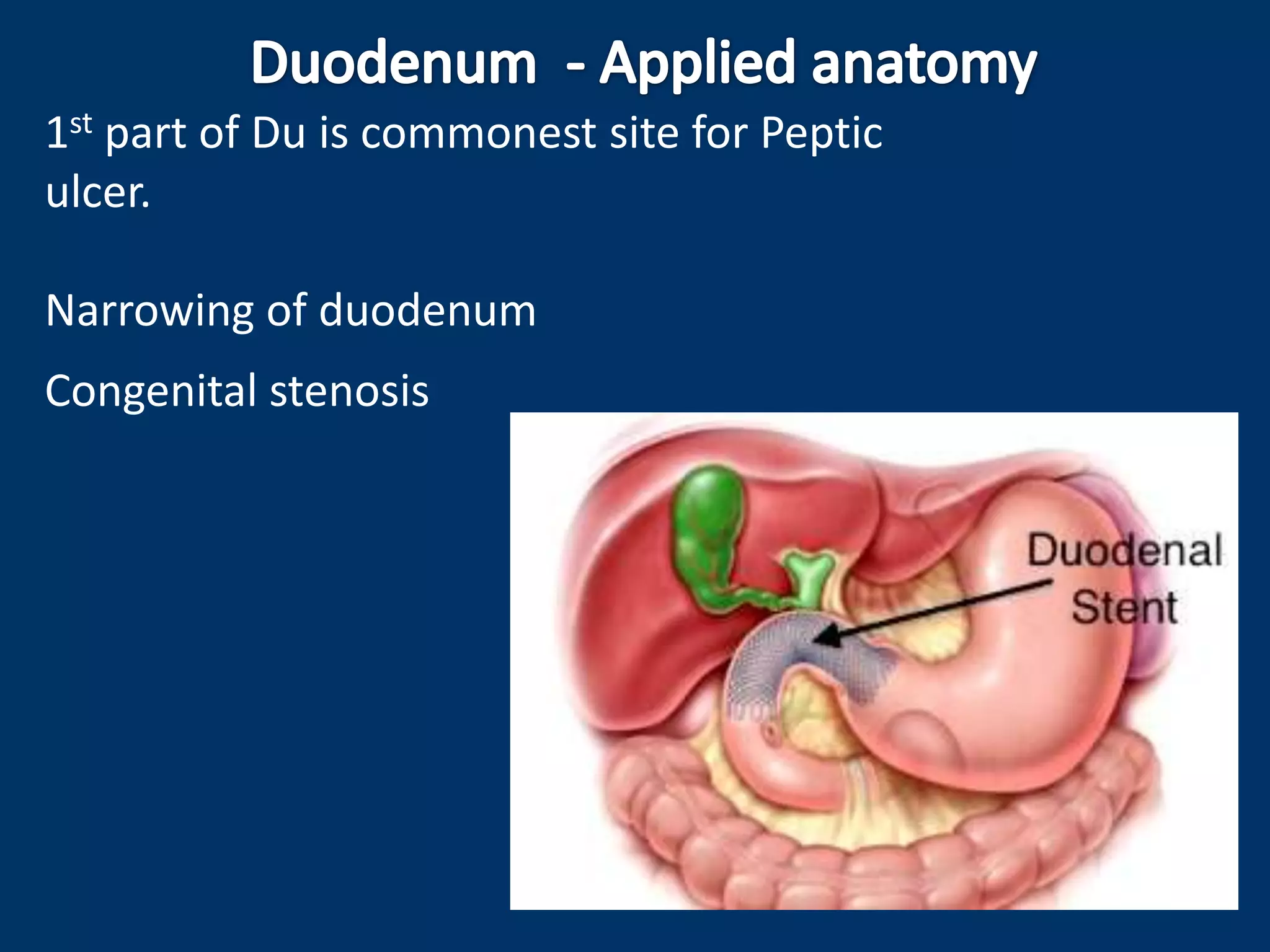
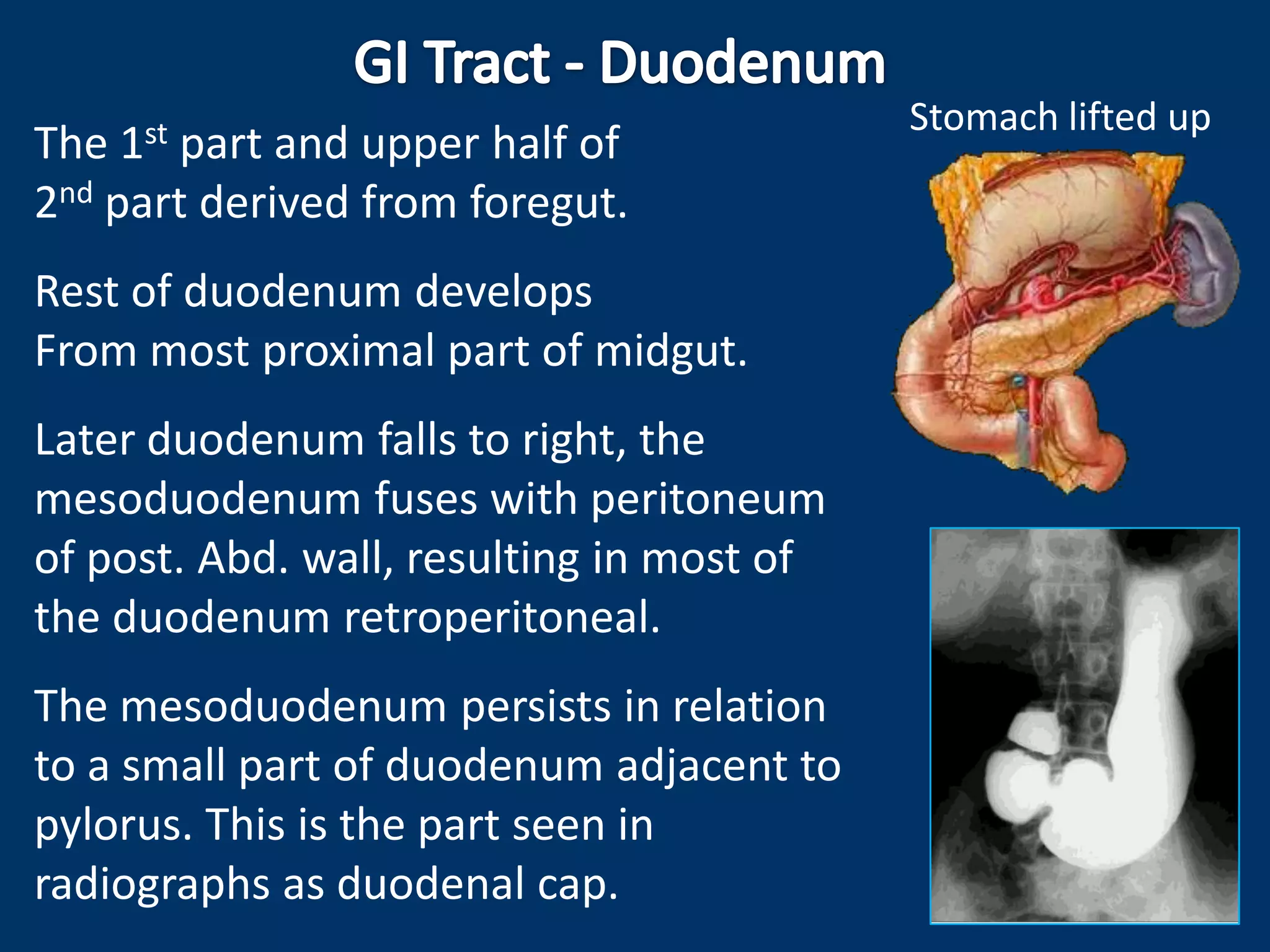
The duodenum is the C-shaped first part of the small intestine. It has four parts and is fixed to the posterior abdominal wall. The first part is the most movable and is a common site for peptic ulcers. It receives bile and pancreatic juices through the major duodenal papilla. The duodenum has circular folds and Brunner's glands in its submucosa. It is supplied by various branches of the celiac artery and drains into the portal vein.