The document provides information about acute appendicitis, including:
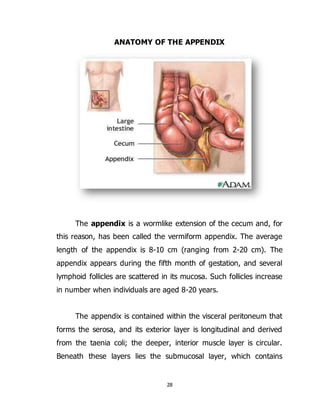
- The appendix is a narrow tube attached to the cecum that contains lymphatic tissue and produces mucus.
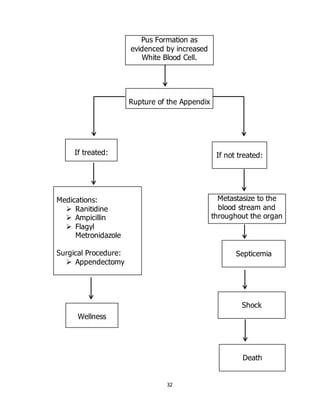
- Acute appendicitis occurs when something blocks the appendix, causing irritation, inflammation, and infection that rapidly grows. Without treatment, the inflamed appendix can rupture.
- Acute appendicitis symptoms include pain in the lower right abdomen that increases with pressure and movement. Left untreated, it can lead to life-threatening complications like abdominal abscesses.
- The document discusses risk factors, symptoms, signs, treatment, and provides a case study of a 23-year-old woman diagnosed with acute appendic





![20
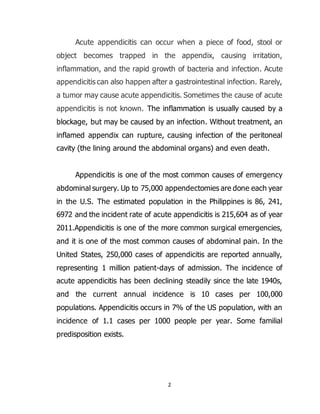
SYMPTOMATOLOGY
Signs and
Symptoms
Present Absent Rationale
Right Lower
Quadrant Pain /
Right lower-quadrant pain that is
produced with either the passive
extension of the patient's right hip
(patient lying on left side, with knee in
flexion) or by the patient's active flexion
of the right hip while supine. The pain
elicited is due to inflammation of the
peritoneum overlying the iliopsoas
muscles and inflammation of the psoas
muscles themselves. Straightening out
the leg causes pain because it stretches
these muscles, while flexing the hip
activates the iliopsoas and therefore also
causes pain.
Source: (http://www.free-
ed.net/sweethaven/science/biology/anat
omyphysiol/Human01_LessonMain.asp?i
Num=1008)
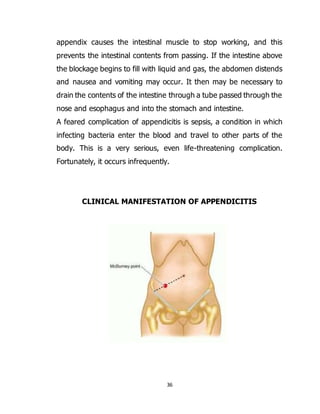
McBurney's Sign
/
Deep tenderness at McBurney's point,
known as McBurney's sign, is a sign
of acute appendicitis.[2]
The clinical sign
of referred pain in the epigastrium when
pressure is applied is also known
as Aaron's sign. Specific localization of
tenderness to McBurney's point indicates
that inflammation is no longer limited to
the lumen of the bowel (which localizes
pain poorly), and is irritating the lining of
the peritoneum at the place where the
peritoneum comes into contact with the](https://image.slidesharecdn.com/88887820-a-case-study-on-acute-appendicitis-150908151643-lva1-app6892/85/88887820-a-case-study-on-acute-appendicitis-20-320.jpg)