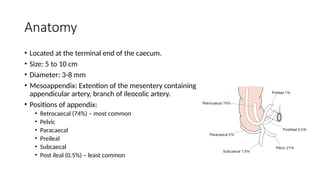
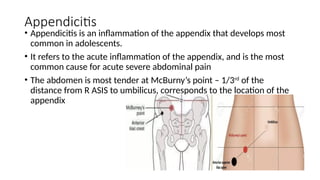
The document provides an overview of appendicitis, detailing its anatomy, causes, clinical features, and types, along with risk factors and differential diagnoses. It discusses the Alvarado score for diagnosing acute appendicitis, various investigation methods like ultrasound and CT scans, and treatment options including surgical interventions. Complications such as appendicular mass and abscess are also addressed, including their clinical features and management approaches.