Downloaded 29 times



![BED: Formula
BED=nd(1+d/[α/β]) - loge2 (T-Tk)/αTp
• n fractions of
• d Gy are given
• in an overall time of T days
• and tumour repopulation doesn’t start until day Tk
(using k for kick-off, or onset, of the delayed
repopulation during fractionated irradiation)
• assuming a constant repopulation rate or cell
doubling time Tp up to the end of the RT](https://image.slidesharecdn.com/normalorganbioogicaleffectivedose-azmalsujamila-151117073557-lva1-app6891/75/Normal-organ-biological-effective-dose-azmal-su-jamila-4-2048.jpg)











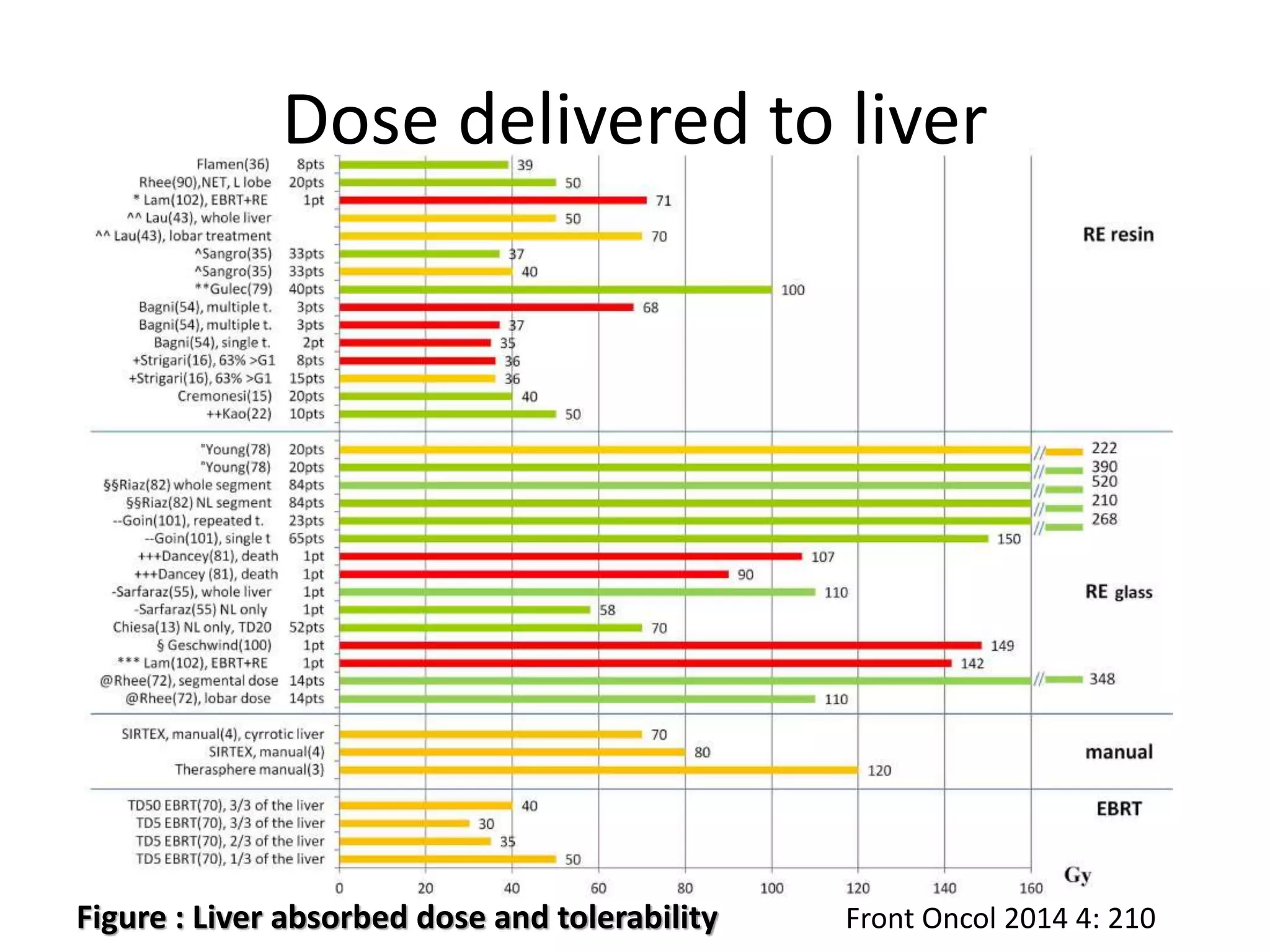







This document discusses the concept of biological effective dose (BED) which is a radiobiological model used to predict clinical outcomes when radiation treatment parameters are altered. It defines BED and provides the formula. It also discusses α and β values, dose limiting organs for various radiopharmaceutical therapies, and safety measures and dose limits reported in literature to protect organs like the kidney, liver, lung, and bone marrow.






















































































