Downloaded 47 times





![72 Nuclear Medicine: The Requisites
from the 4-hour value to plan the therapy I-131 dose.
However, some patients have rapid thyroid iodine turn-
over. These patients may show a very high 4- to 6-hour
%RAIU but much lower values at 24 hours, perhaps only
mildly elevated (Fig. 6-4). Therefore the more accurate
24-hour measurement certainly needs to be used for ther-
apy dose calculated from a 24-hour %RAIU whenever
early values are markedly elevated.
Technetium-99m Pertechnetate Uptake
A Tc-99m pertechnetate uptake is not commonly per-
formed. Advantages over a %RAIU are that the study can
be completed within 20 to 30 minutes and radioiodine is
not needed. The disadvantages include much lower accu-
racy than the %RAIU and a lack of widespread commercial
software for Tc-99m pertechnetate calculation. In addi-
tion, the lack of organification prevents accurate measure-
ment of the 24-hour %RAIU, standard practice for I-131
therapy dose calculation.
Methodology. A gamma camera imaging technique is
used rather than a scintillation probe because of the high
neck background. Before and after injection of the Tc-
99m, the syringe is imaged (preinjection counts − postin-
jection residual counts = administered counts). Images are
acquired on a computer. Regions of interest are drawn on a
computer for the thyroid, thyroid background, and
syringes. Areas of interest are normalized for pixel size,
and thyroid and syringe counts are normalized for time of
acquisition. Normal Tc-99m uptake is 0.3% to 4.5%.
Thyroid Scan
Thyroid scintigraphy depicts the entire gland in a single
image and allows direct correlation of physical findings with
abnormalities in the image. The combination of gamma
camera and pinhole collimator makes possible multiple-
view high-resolution images of the thyroid. Pinhole colli-
mator magnification provides image resolution superior to
parallel-hole collimators, approximately 5 mm compared to
more than 1.5 cm with a parallel-hole collimator (Fig. 6-7).
The thyroid gland should be routinely examined by pal-
pation at the time of imaging, to estimate gland size and
confirm the presence and location of nodules. A radioactive
marker source (122-keV cobalt-57 or Tc-99m) or lead can
be used to correlate thyroid palpation findings with the
scintigraphic image. Other imaging modalities performed
before the scan (e.g., sonography, computed tomography
[CT]) should always be reviewed.
Methodology
Iodine-123 and Technetium-99m Pertechnetate
Scintigraphy. For an I-123 scan, the patient ingests 300
to 400 μCi orally. The scan is usually acquired 4 hours later.
It may be more convenient to perform the scan at the same
time as the 24-hour %RAIU. However, the low count rate
at 24 hours requires longer acquisition time, which
increases the likelihood of patient movement. Images can
be acquired at 4 hours for a shorter time, and image quality
is far superior. For a Tc-99m pertechnetate scan, 3 to 5 mCi
is administered intravenously. Imaging begins 20 minutes
after injection. Early imaging is required because Tc-99m
is not organified and thus not retained within the thyroid.
For both radiopharmaceuticals, a large field-of-view
gamma camera is equipped with a pinhole collimator that
has an interchangeable lead pinhole insert of 3- to 6-mm in
internal diameter placed in its distal aspect. Smaller diam-
eter inserts provide higher resolution but lower sensitivity
for count detection. A 4-mm insert is commonly used.
A 15% to 20% photopeak window is centered at 159
keV for I-123 and at 140 keV for Tc-99m. Imaging proto-
cols for the two radiopharmaceuticals are otherwise simi-
lar and described in more detail in Box 6-3. The patient is
positioned supine with the neck hyperextended and the
plane of the thyroid gland roughly parallel to the crystal
face of the camera. The gland should fill approximately
two thirds of the field of view. This is achieved by placing
the collimator 6 to 8 cm from the surface of the neck. Col-
limator magnification increases as the pinhole approaches
the neck.
On one image, a radioactive marker (Tc-99m, Co-57) or
computer cursor is routinely placed at the sternal notch and
right side. For this image, the collimator could be placed at
a greater distance to the neck, resulting in a smaller thyroid
image (Fig. 6-8). In some clinics, a line source marker or
two point sources 4 or 5 cm apart are placed on the neck
lateral to the thyroid lobes and parallel to their long axis to
estimate the size of the thyroid and nodules.
Images are routinely obtained in the anterior, right ante-
rior oblique, and left anterior oblique views. Each image is
acquired for approximately 100,000 counts or 5 to 7 minutes.
It is preferable for the patient to remain in one position
while the camera and collimator are moved to the different
projections,thusmakingimagesmorereproduciblebetween
patient and resulting in less image distortion and patient
motion.
Additional images using a radioactive marker can help
determine whether a palpable nodule takes up the
Figure 6-7. Pinhole collimator. The pinhole collimator is attached to
the front of the gamma camera and positioned close to the thyroid to
permit optimal magnification. If positioned farther away, the resulting
image would be smaller.](https://image.slidesharecdn.com/6endocrine-141117030144-conversion-gate02/85/6-endocrine-7-320.jpg)









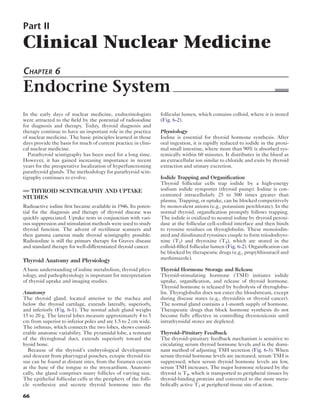
![Endocrine System 83
Figure 6-22. Substernal goiter with I-123 hybrid SPECT/CT. The I-123 thyroid scan is fused with the CT scan in selected transverse, sagittal, and
coronal views. This patient had a multinodular toxic goiter with substernal extension.
Figure 6-23. Lingual thyroid. Hypothyroid infant with neck mass. Thy-
roid scan (anterior view) shows prominent uptake within the midline
neck mass. There is no thyroid uptake in the region of thyroid bed.
Box 6-6. Indications for Iodine-131 Therapy
INDICATED
Graves disease (diffuse toxic goiter)
Plummer disease (toxic nodules)
Functioning thyroid cancer (metastatic)
NOT INDICATED
Thyrotoxicosis factitia
Subacute thyroiditis
“Silent” thyroiditis (atypical, subacute, lymphocytic,
transient, postpartum)
Struma ovarii
Thyroid hormone resistance (biochemical or
clinical manifestations)
Secondary hyperthyroidism (pituitary tumor,
ectopic thyroid-stimulating hormone, trophoblastic
tumors [human chorionic gonadotropin])
Thyrotoxicosis associated with Hashimoto disease
(hashitoxicosis)
Jod-Basedow phenomenon (iodine-induced
hyperthyroidism)](https://image.slidesharecdn.com/6endocrine-141117030144-conversion-gate02/85/6-endocrine-18-320.jpg)
![84 Nuclear Medicine: The Requisites
Graves Disease
Patients with newly diagnosed Graves disease are often ini-
tially treated with beta-blockers for symptomatic relief and
more specific therapy with thiourea antithyroid drugs (e.g.,
propylthiouracil [PTU] and methimazole [Tapazole]), which
block organification and reduce thyroid hormone production.
These drugs “cool” the patient down and render the patient
euthyroid, providing time to consider further therapeutic
options. Patients may be instructed to take these drugs for 6
to 12 months. However, the drugs have a high incidence of
adverse effects (50%), the most serious being liver dysfunc-
tion and agranulocytosis. Thus they are rarely prescribed for
longer than a year. Thyroidectomy is an uncommon therapy
and associated with significant risk. Most patients ultimately
receive radioiodine I-131 therapy. Increasingly patients are
being treated with I-131 soon after diagnosis.
The exophthalmos of Graves disease is not controlled
by thiourea antithyroid drugs or I-131 therapy. Some evi-
dence even suggests that exacerbation of exophthalmos
may occur with I-131 therapy; thus corticosteroids may be
administered concomitantly.
Most patients with Graves disease are effectively treated
with one therapeutic dose of I-131. The patient usually
notes symptomatic improvement within 3 weeks of ther-
apy; however, the full therapeutic effect takes 3 to 6
months because stored hormone must first be released.
Radioiodine therapy may not initially be effective in up to
10% of patients. They require repeat treatment, usually
with a higher administered dose.
Pregnancy must be excluded before I-131 therapy is
administered. Women should be counseled to avoid preg-
nancy for 3 to 6 months after therapy in the event that
retreatment is necessary.
Many decades of experience with therapeutic I-131
have shown it to be safe and effective. Endocrinologists
have become comfortable with treating patients, even
children, with I-131 because of its high efficacy and low
incidence of acute or chronic adverse effects.
Most patients treated with I-131 ultimately develop
hypothyroidism and require replacement hormone ther-
apy. This may occur as early as several months after ther-
apy or may take decades. With a larger administered dose,
the likelihood increases for early onset of hypothyroidism.
With a lower administered dose, the likelihood of disease
recurrence is higher.
Occasional patients develop radiation thyroiditis after
I-131 therapy, causing local neck pain, tenderness, or
swelling. Very rarely, this can result in thyroid storm. It is
important to recognize this serious complication, which
may require hospitalization and steroid therapy. Patients
in a very toxic state and those treated with higher amounts
of radioactivity are at greater risk. Beta-blockers used
before and after therapy can minimize this risk.
Evidence over many decades of I-131 therapy has not
shown a statistically significant increase in the frequency of
secondary cancers, infertility, or congenital defects in chil-
dren of patients receiving I-131 therapy for Graves disease.
Iodine-131 Dose Selection
Various approaches have been used for selecting an I-131
dose for therapy in patients with Graves disease. One
method is to prescribe standard I-131 dose in the range of
8 to 15 mCi. This often works. However, factors such as the
size of the gland and %RAIU may result in very different
radiation doses to the thyroid across patients. Large glands
require a relatively higher therapeutic dose, and patients
with a high %RAIU need a lower dose. Some radiothera-
pists adjust this dose based on these two factors.
Another common approach is to use a standard formula that
takes gland size, the %RAIU, and the proposed administered
I-131 dose per gram of thyroid tissue into consideration:
I-131 administered dose =
Gram size of thyroid gland ×
100−thiourea 180 μCi/g
24-hour %RAIU
This approach calculates an individual therapy dose for
each patient with Graves disease. See example (Box 6-7). An
estimation of the gram weight of the gland is required. A nor-
mal gland weighs 15 to 20 g. Patients with Graves disease
typically have glands in the range of 40 to 80 g but sometimes
considerably larger. Considerable interphysician variability
exists in estimation of gland size by palpation; however, an
experienced physician is able to reproducibly estimate gland
size. The size of larger glands is often underestimated.
Another variable in this calculation is the microcurie per
gram dose. In the past, referring physicians often requested
low I-131 doses to minimize the radiation to the patient
(e.g., 60-80 μCi/g tissue). Today, referring physicians are
more comfortable with the safety of higher doses (120-180
μCi/g tissue) and often prefer the higher likelihood of suc-
cess with a single therapeutic dose. Early-onset hypothy-
roidism is also often preferred by some physicians because
they feel it is inevitable and prompt replacement therapy
can be instituted.
Patients with rapid radioiodine turnover in the gland
(e.g., high 4-hour but normal or near-normal 24-hour
%RAIU) have a shorter I-131 thyroid residence time. Thus
a higher I-131 dose than would be calculated using the
standard 24-hour %RAIU should be considered.
Toxic Nodular Disease
Toxic nodules are more resistant to therapy with radioio-
dine than Graves disease. The reason is unclear, but it may
be that I-131 thyroid residence time in the nodule(s) is
reduced, leading to a lower retained dose. The adminis-
tered I-131 therapeutic dose is often increased by 50% over
what would be prescribed for Graves disease. An empirical
dose of 20 to 25 mCi is also often used. Because extranodu-
lar tissue is suppressed and spared from radiation, normal
function usually resumes after successful therapy.
Thyroid Cancer
Well-differentiated thyroid cancer originates from thyroid
follicular epithelium and retains biological characteristics
of healthy thyroid tissue, including expression of the
sodium iodide symporter, which is responsible for radioio-
dine uptake. The prognosis with appropriate treatment is
generally good, with an estimated 10-year survival rate of
85%. Even with distant metastases, the 10-year survival is
25% to 40%. However, the lifetime recurrence rate is 10%
to 30%, so long-term follow-up is required and subsequent
therapy is necessary for many patients.](https://image.slidesharecdn.com/6endocrine-141117030144-conversion-gate02/85/6-endocrine-19-320.jpg)














This document discusses thyroid scintigraphy and uptake studies using various radiopharmaceuticals. It begins by describing the early use of radioactive iodine in nuclear medicine and its continued importance in thyroid diagnosis and therapy. It then provides details on the anatomy and physiology of the thyroid gland and iodine metabolism. The remainder of the document focuses on the radiopharmaceuticals used in thyroid scintigraphy, including their physical properties, dosimetry considerations, and imaging characteristics. In particular, it compares the properties and use of radioactive iodine isotopes I-123 and I-131 as well as technetium-99m pertechnetate.























































































