Downloaded 17 times







![Brugada P, Brugada J, Mont L, Smeets J, Andries EW. (1991) A new approach to the differential diagnosis of a regular tachycardia with a wide QRS complex. Circulation.
;83:1649–59. [PubMed] [Google Scholar]
Step 1.
Absence of RS](https://image.slidesharecdn.com/ecgvtachbrugadavereckeialgorithm-mecelino-211016123258/75/Ecg-vtach-brugada-amp-vereckei-algorithm-mec-elino-13-2048.jpg)




![Brugada P, Brugada J, Mont L, Smeets J, Andries EW. A new approach to the differential diagnosis of a regular tachycardia with a wide QRS complex. Circulation.
1991;83:1649–59. [PubMed] [Google Scholar]
Step 1. Absence of RS = V T
If RS complex present, Proceed
to Step 2](https://image.slidesharecdn.com/ecgvtachbrugadavereckeialgorithm-mecelino-211016123258/75/Ecg-vtach-brugada-amp-vereckei-algorithm-mec-elino-18-2048.jpg)
![Brugada P, Brugada J, Mont L, Smeets J, Andries EW. A new approach to the differential diagnosis of a regular tachycardia with a wide QRS complex. Circulation.
1991;83:1649–59. [PubMed] [Google Scholar]
Step 2.
Is the R to S greater than 100ms?](https://image.slidesharecdn.com/ecgvtachbrugadavereckeialgorithm-mecelino-211016123258/75/Ecg-vtach-brugada-amp-vereckei-algorithm-mec-elino-19-2048.jpg)
![Brugada P, Brugada J, Mont L, Smeets J, Andries EW. A new approach to the differential diagnosis of a regular tachycardia with a wide QRS complex. Circulation.
1991;83:1649–59. [PubMed] [Google Scholar]
Step 2.
Is the R to S greater than 100ms?
Brugada Sign:
q to nadir of S > 100ms
Josephson
Sign: slurring of S
wave](https://image.slidesharecdn.com/ecgvtachbrugadavereckeialgorithm-mecelino-211016123258/75/Ecg-vtach-brugada-amp-vereckei-algorithm-mec-elino-20-2048.jpg)

![Brugada P, Brugada J, Mont L, Smeets J, Andries EW. A new approach to the differential diagnosis of a regular tachycardia with a wide QRS complex. Circulation.
1991;83:1649–59. [PubMed] [Google Scholar]
Step 2.
Is the R to S greater than 100ms?
If not, proceed to Step 3.](https://image.slidesharecdn.com/ecgvtachbrugadavereckeialgorithm-mecelino-211016123258/75/Ecg-vtach-brugada-amp-vereckei-algorithm-mec-elino-23-2048.jpg)
![Brugada P, Brugada J, Mont L, Smeets J, Andries EW. A new approach to the differential diagnosis of a regular tachycardia with a wide QRS complex. Circulation.
1991;83:1649–59. [PubMed] [Google Scholar]
Step 3.
Is there AV dissociation?](https://image.slidesharecdn.com/ecgvtachbrugadavereckeialgorithm-mecelino-211016123258/75/Ecg-vtach-brugada-amp-vereckei-algorithm-mec-elino-24-2048.jpg)





![Brugada P, Brugada J, Mont L, Smeets J, Andries EW. A new approach to the differential diagnosis of a regular tachycardia with a wide QRS complex. Circulation.
1991;83:1649–59. [PubMed] [Google Scholar]
Step 4.
Look for the Morphology Criteria](https://image.slidesharecdn.com/ecgvtachbrugadavereckeialgorithm-mecelino-211016123258/75/Ecg-vtach-brugada-amp-vereckei-algorithm-mec-elino-30-2048.jpg)





![Vereckei A, Duray G, Szénási G, Altemose GT, Miller JM. A new algorithm using only lead aVR for the differential diagnosis of
wide QRS complex tachycardia. Heart Rhythm. 2008;5:89–98. [PubMed] [Google Scholar]
Step 1.
Initial R wave in aVR](https://image.slidesharecdn.com/ecgvtachbrugadavereckeialgorithm-mecelino-211016123258/75/Ecg-vtach-brugada-amp-vereckei-algorithm-mec-elino-36-2048.jpg)


![Vereckei A, Duray G, Szénási G, Altemose GT, Miller JM. A new algorithm using only lead aVR for the differential diagnosis of
wide QRS complex tachycardia. Heart Rhythm. 2008;5:89–98. [PubMed] [Google Scholar]
Step 1.
Initial R wave in aVR
Present in our ECG](https://image.slidesharecdn.com/ecgvtachbrugadavereckeialgorithm-mecelino-211016123258/75/Ecg-vtach-brugada-amp-vereckei-algorithm-mec-elino-39-2048.jpg)
![Vereckei A, Duray G, Szénási G, Altemose GT, Miller JM. A new algorithm using only lead aVR for the differential diagnosis of
wide QRS complex tachycardia. Heart Rhythm. 2008;5:89–98. [PubMed] [Google Scholar]
If there is no
Initial R wave in aVR
Assess the width of
initial r wave or q wave > 40ms](https://image.slidesharecdn.com/ecgvtachbrugadavereckeialgorithm-mecelino-211016123258/75/Ecg-vtach-brugada-amp-vereckei-algorithm-mec-elino-40-2048.jpg)
![Vereckei A, Duray G, Szénási G, Altemose GT, Miller JM. A new algorithm using only lead aVR for the differential diagnosis of
wide QRS complex tachycardia. Heart Rhythm. 2008;5:89–98. [PubMed] [Google Scholar]
If the width of
initial r wave or q wave
doesn’t reach 1 small box
(40ms)
see the notching of initial downstroke](https://image.slidesharecdn.com/ecgvtachbrugadavereckeialgorithm-mecelino-211016123258/75/Ecg-vtach-brugada-amp-vereckei-algorithm-mec-elino-41-2048.jpg)
![Vereckei A, Duray G, Szénási G, Altemose GT, Miller JM. A new algorithm using only lead aVR for the differential diagnosis of
wide QRS complex tachycardia. Heart Rhythm. 2008;5:89–98. [PubMed] [Google Scholar]
If there’s no notching of
QRS downstroke
Compute for V initial / V terminal
A value of lesser than 1 = V
Tach](https://image.slidesharecdn.com/ecgvtachbrugadavereckeialgorithm-mecelino-211016123258/75/Ecg-vtach-brugada-amp-vereckei-algorithm-mec-elino-42-2048.jpg)



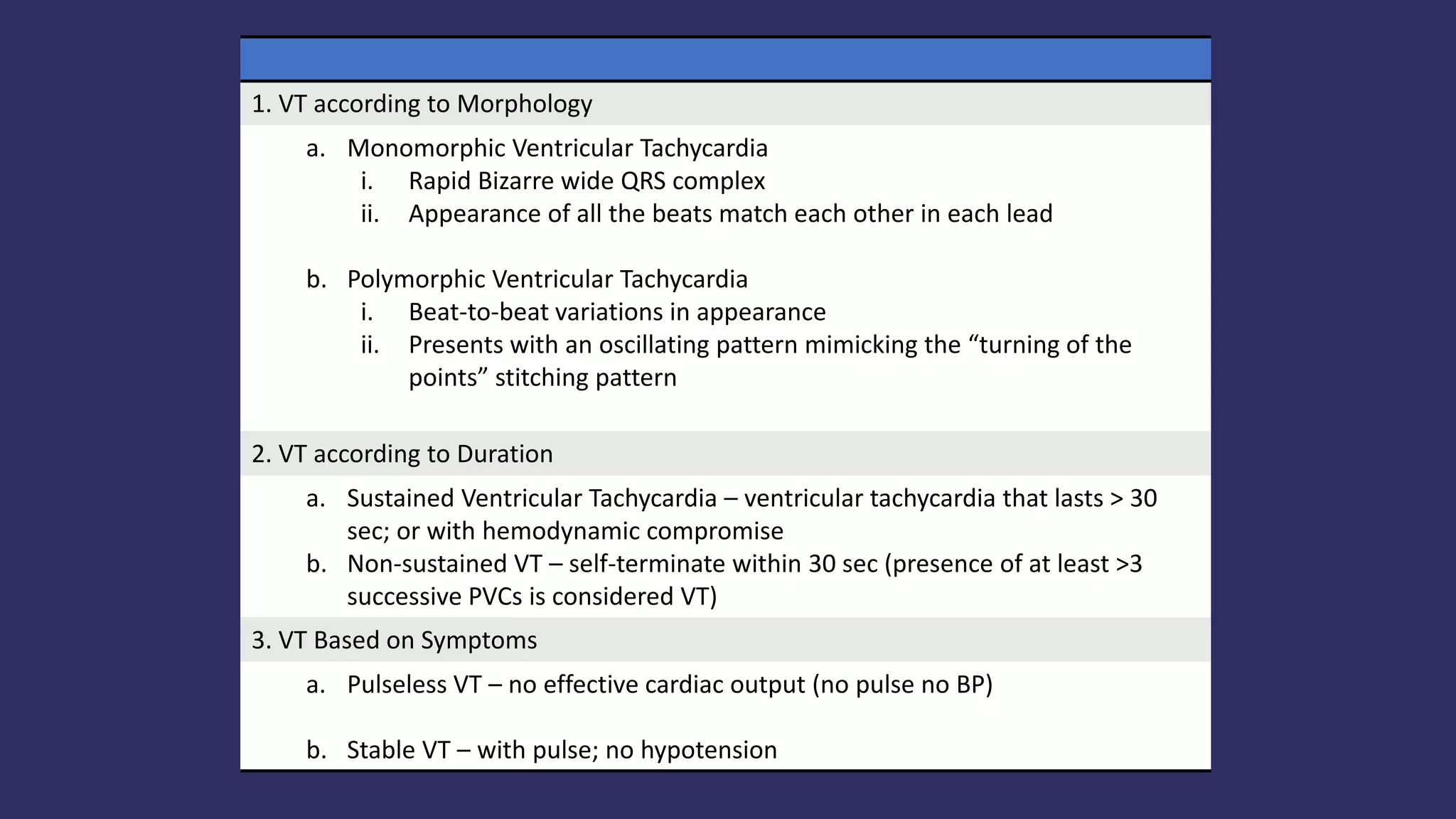


This document summarizes diagnostic algorithms for ventricular tachycardia (VT), including the Brugada algorithm and Vereckei algorithm. The Brugada algorithm uses three steps - absence of RS complex, R-S interval over 100ms, and checking for AV dissociation. The Vereckei algorithm only uses lead aVR and analyzes initial R wave dominance, QRS width over 40ms, notching, and V initial/V terminal ratio. The document also discusses differentiating VT from supraventricular tachycardia with aberrancy based on morphology, duration, and symptoms.























































































