Downloaded 11 times
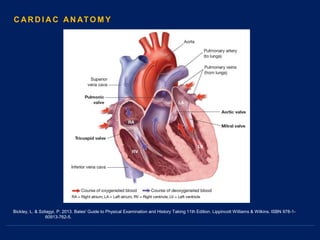
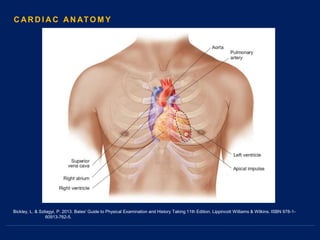
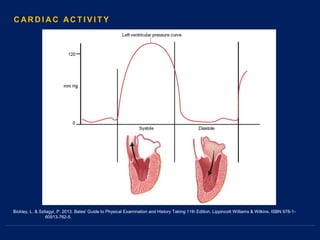
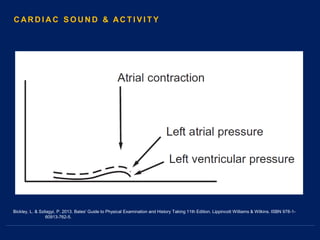
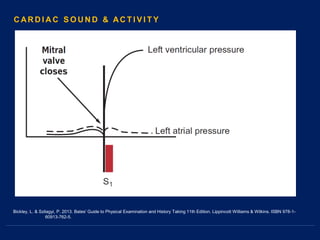
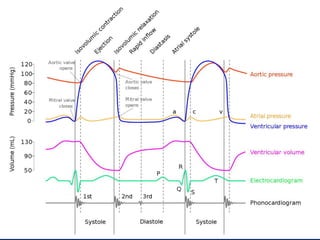
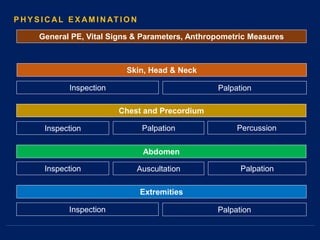
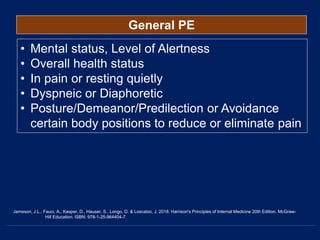
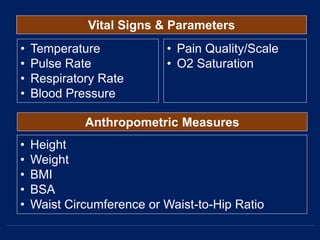
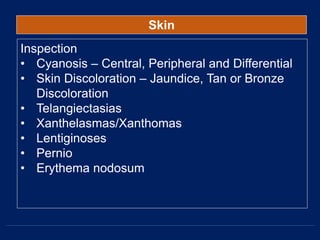



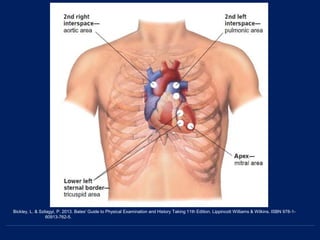
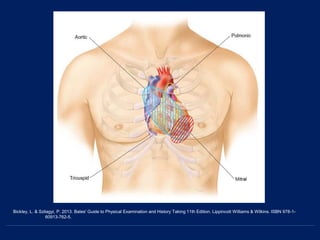
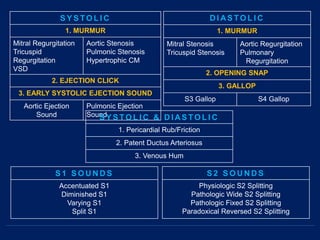
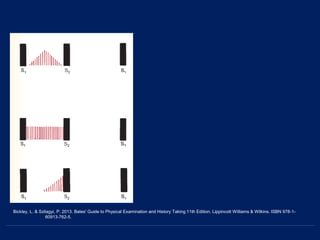


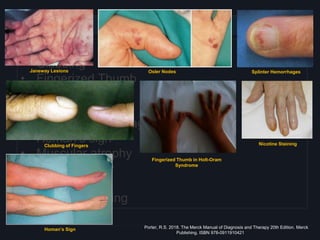
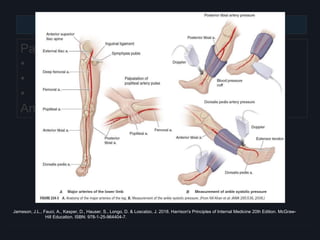
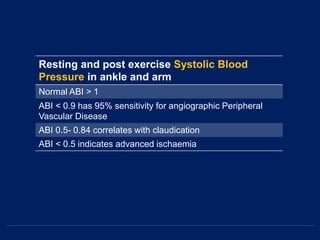
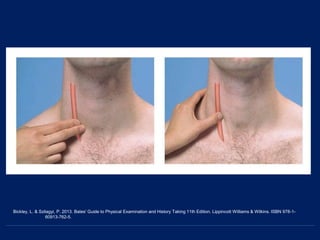
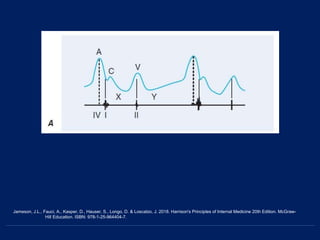
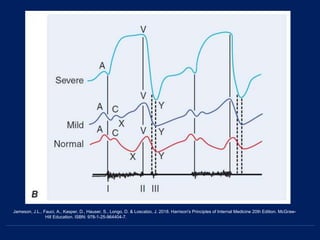
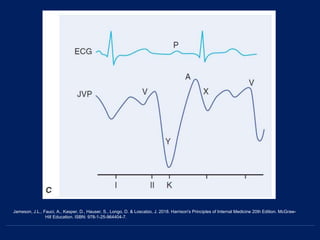

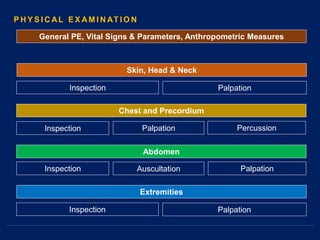

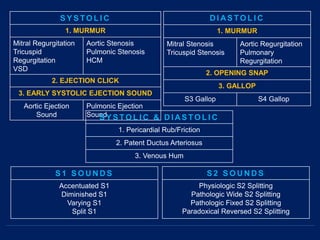
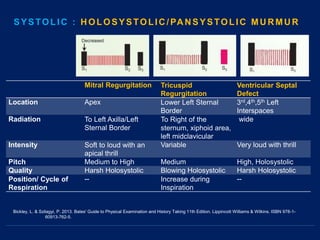
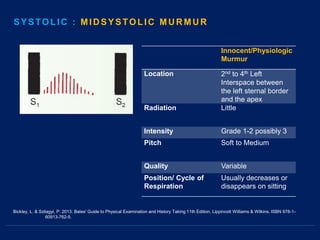
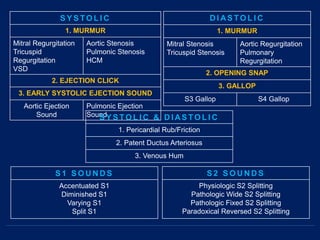
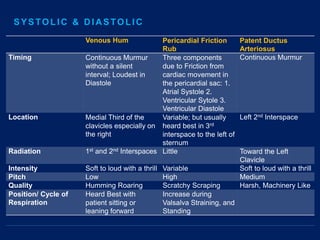
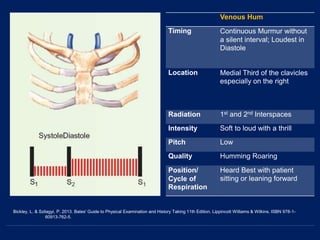
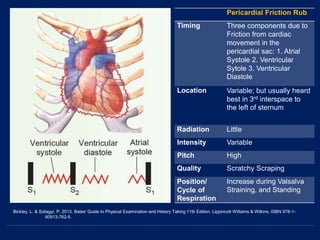
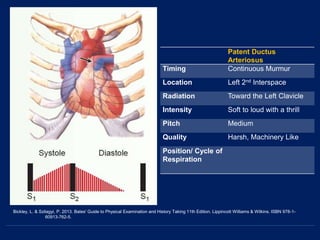
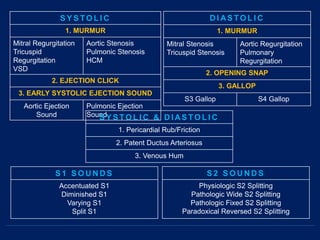
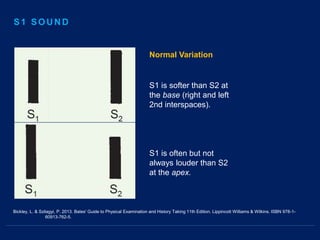
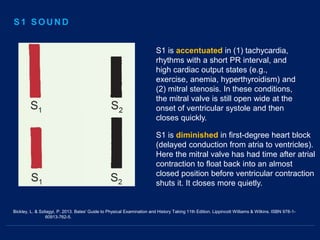

This document provides an outline for a physical examination focused on cardiovascular health. It begins with an introduction on cardiac anatomy, sounds, and conduction. The physical examination section describes inspecting, palpating, and auscultating the skin, head, neck, chest, abdomen, and extremities. Vital signs and common findings are also reviewed, including assessing jugular venous distention and lymph nodes in the neck. Key cardiac sounds and murmurs are defined. References include textbooks on internal medicine, physical examination, and cardiology.























































































