Downloaded 873 times


![BMS vs DES -G2
Cobalt-chromium everolimus-eluting stents (CoCr-EES)
• one-year risk of cardiac death/ MI was reduced with the former but not
the latter (odds ratio [OR] 0.63, 95% CI 0.42-0.92 and 0.86, 95% CI 0.50-
1.49).
• one-year risk TVR was reduced with the former but not the latter (OR 0.45,
95% CI 0.29-0.66 and 0.60, 95% CI 0.34-1.05).
• the one-year risk of definite stent thrombosis was reduced with the
former but not the latter (OR 0.32, 95% CI 0.11-0.78 and 0.44, 95% CI 0.12-
1.79).
• lower one-year rates of cardiac death or MI, definite stent thrombosis, and
target vessel revascularization](https://image.slidesharecdn.com/primarypci-130928132211-phpapp01/85/Primary-Percutaneus-coronary-intervention-46-320.jpg)





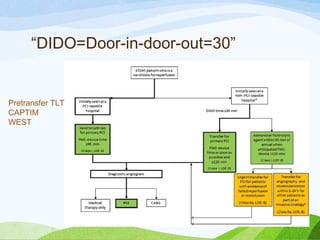
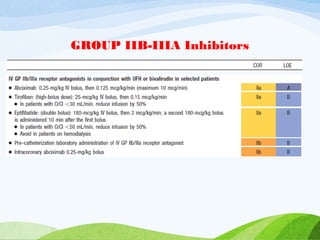
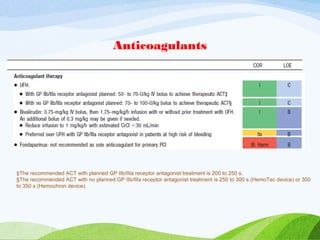
Primary PCI involves performing urgent angioplasty and potentially stenting of the culprit artery in STEMI patients, with the goal of reopening the blocked vessel within 90 minutes of first medical contact. It is the preferred reperfusion strategy when it can be performed promptly by an experienced team. Factors such as patient age, time to treatment, comorbidities, and initial flow in the artery help determine whether primary PCI or thrombolysis is most appropriate. Optimal anticoagulation and antiplatelet regimens along with adjunctive therapies like manual thrombectomy can improve outcomes of primary PCI.























































































