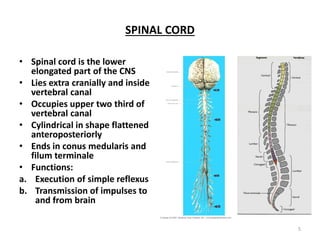
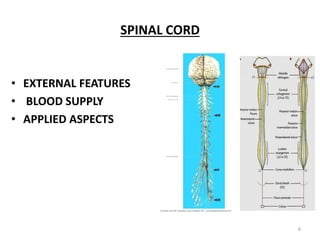
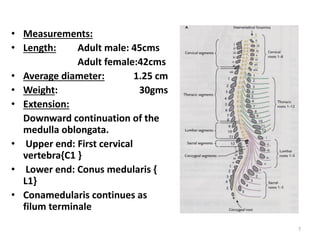
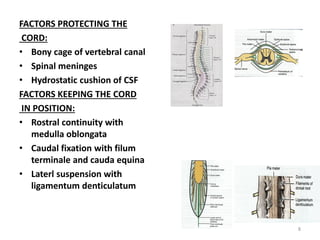
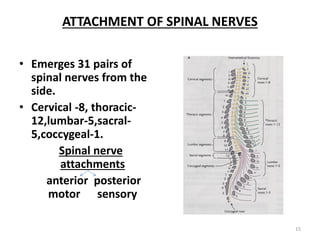
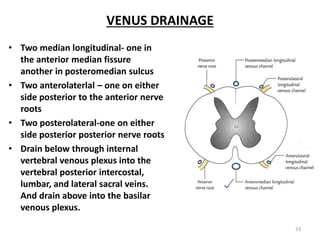
The spinal cord is the lower elongated part of the central nervous system that lies extra cranially within the vertebral canal. It extends from the foramen magnum to the lower border of L1 vertebra. The spinal cord has 31 pairs of spinal nerves that emerge from it and it is protected within the bony vertebral canal by the meninges. It receives its blood supply from the anterior and posterior spinal arteries as well as segmental medullary branches. Injuries and diseases of the spinal cord can result in various clinical manifestations depending on the location and severity of the lesion.