Downloaded 1,328 times
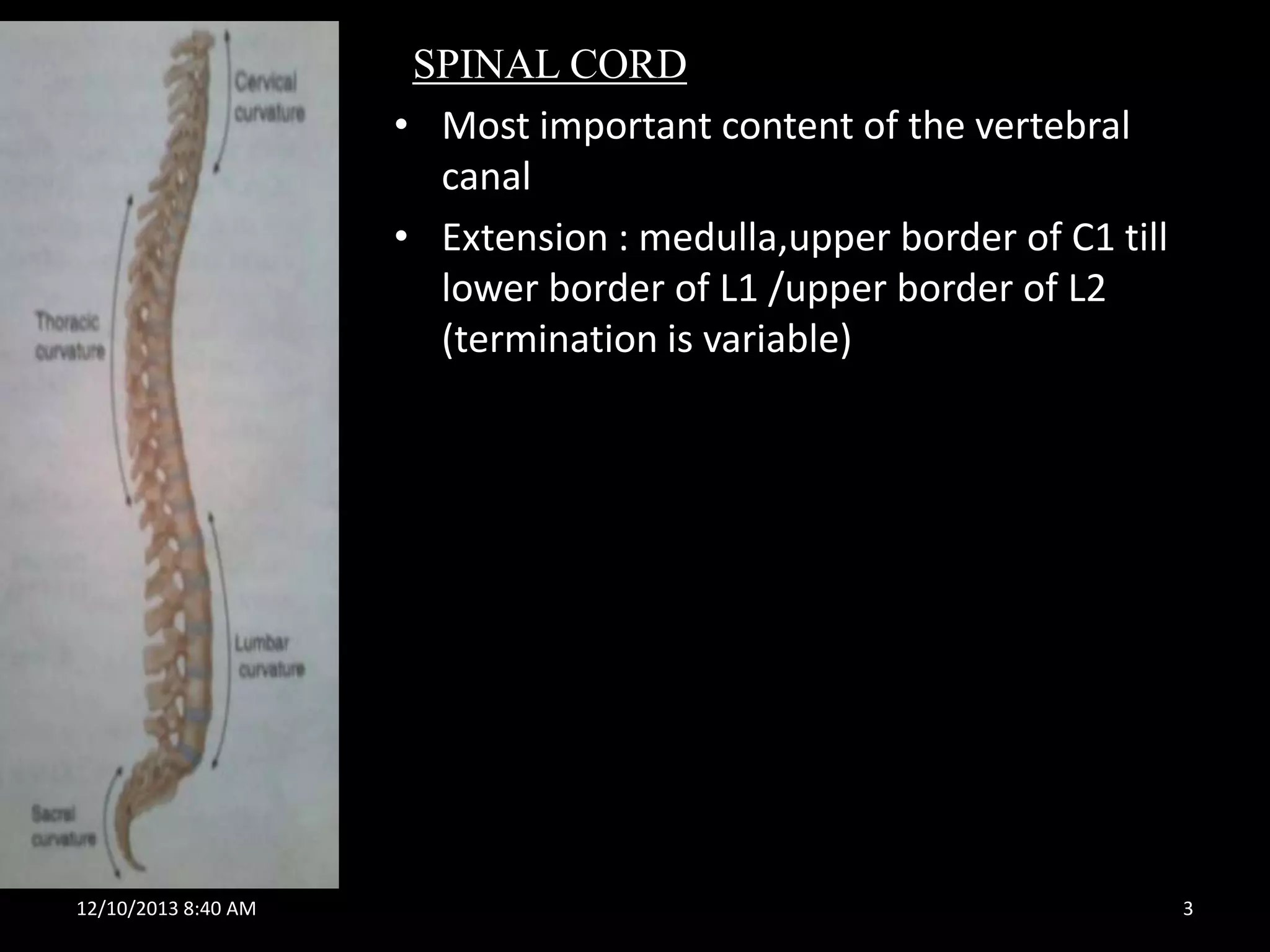
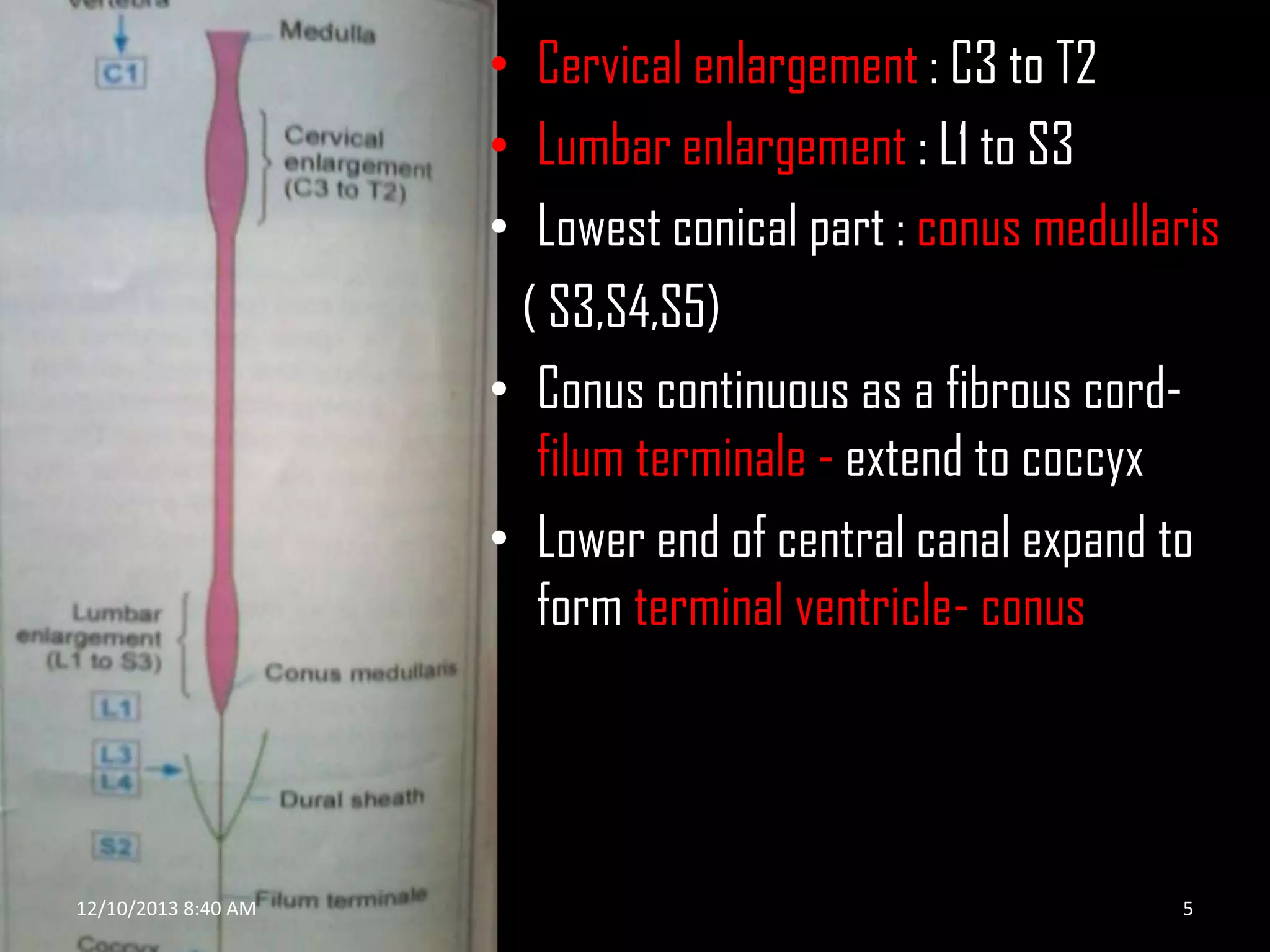
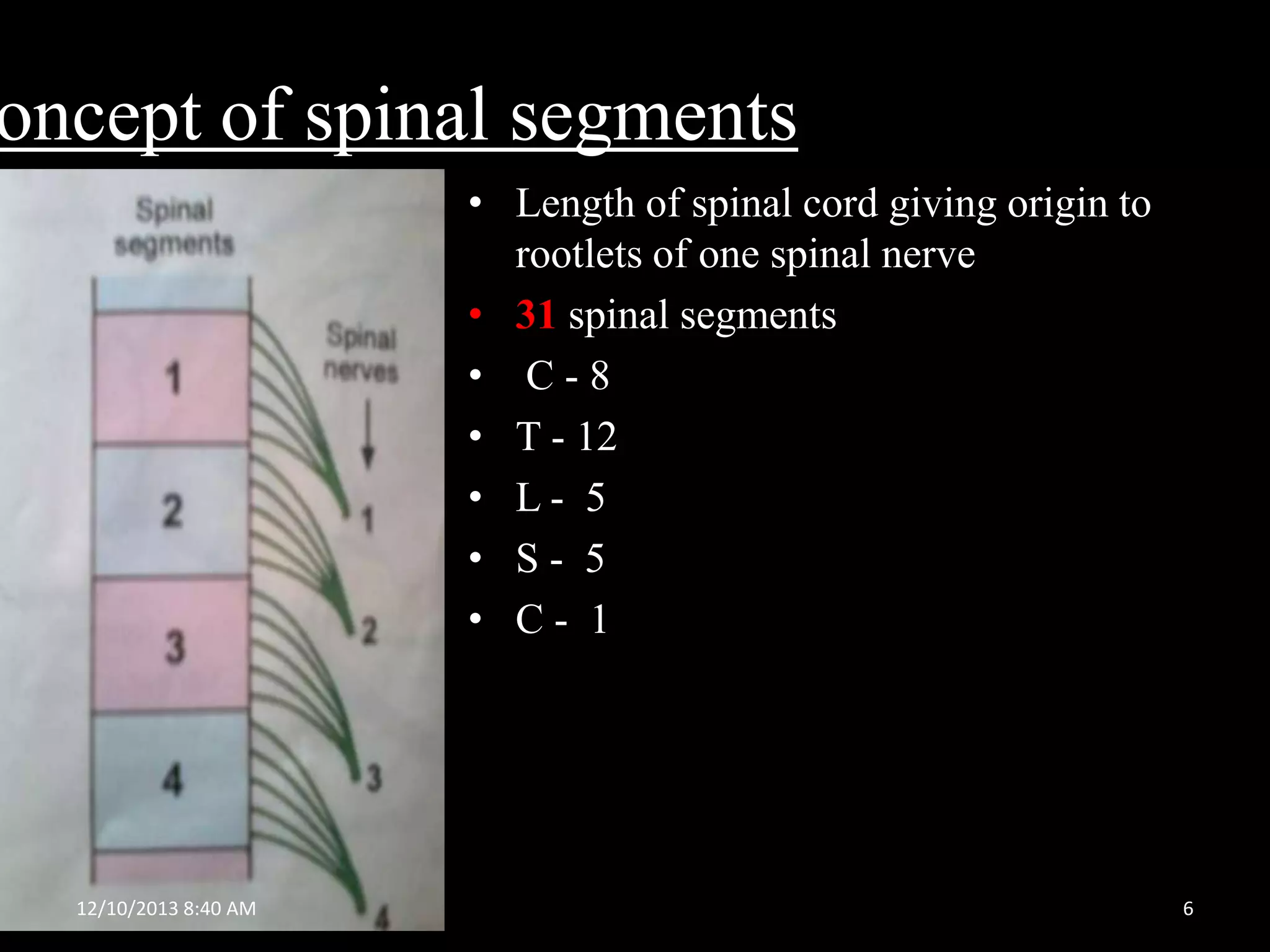
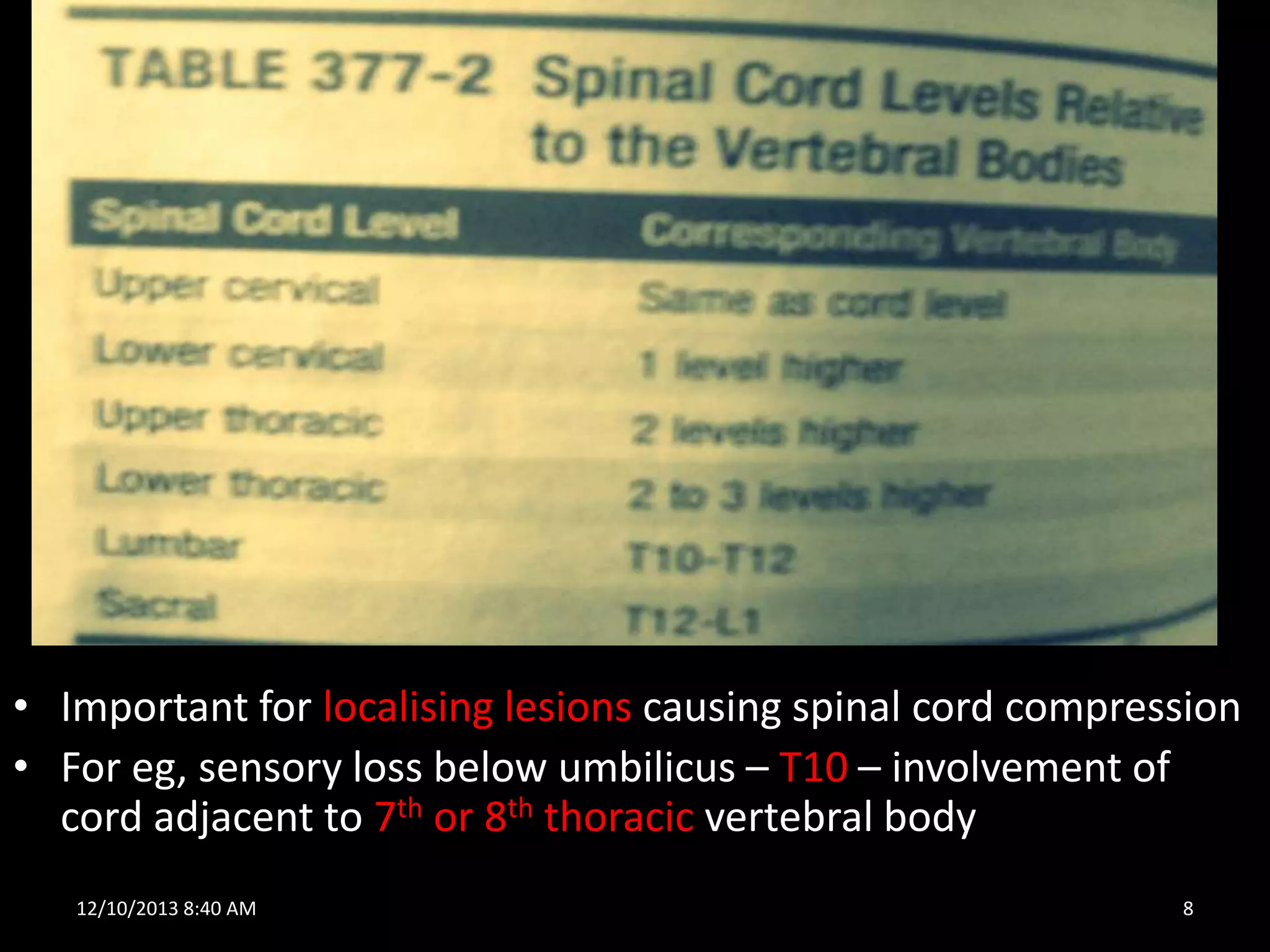
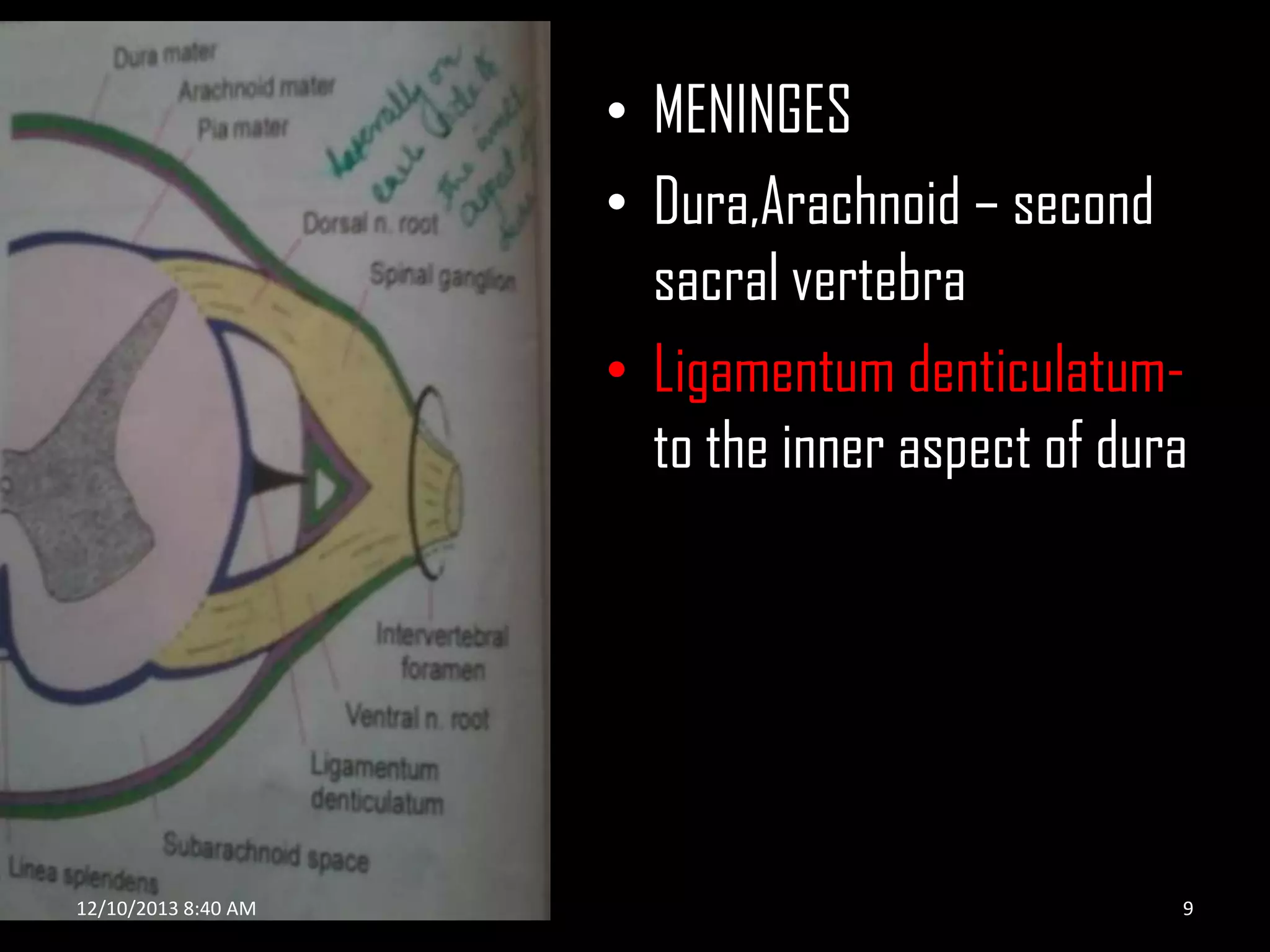
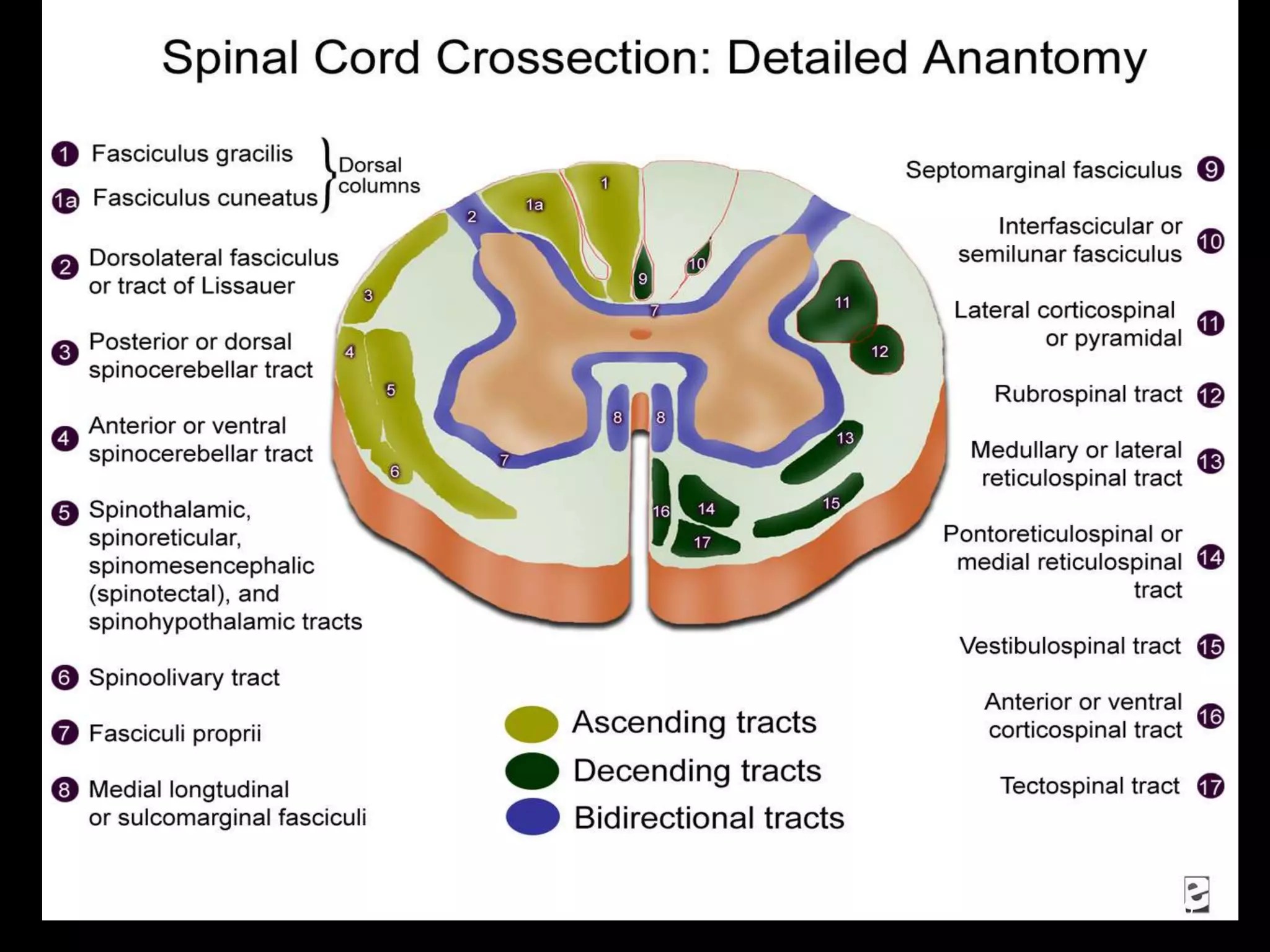
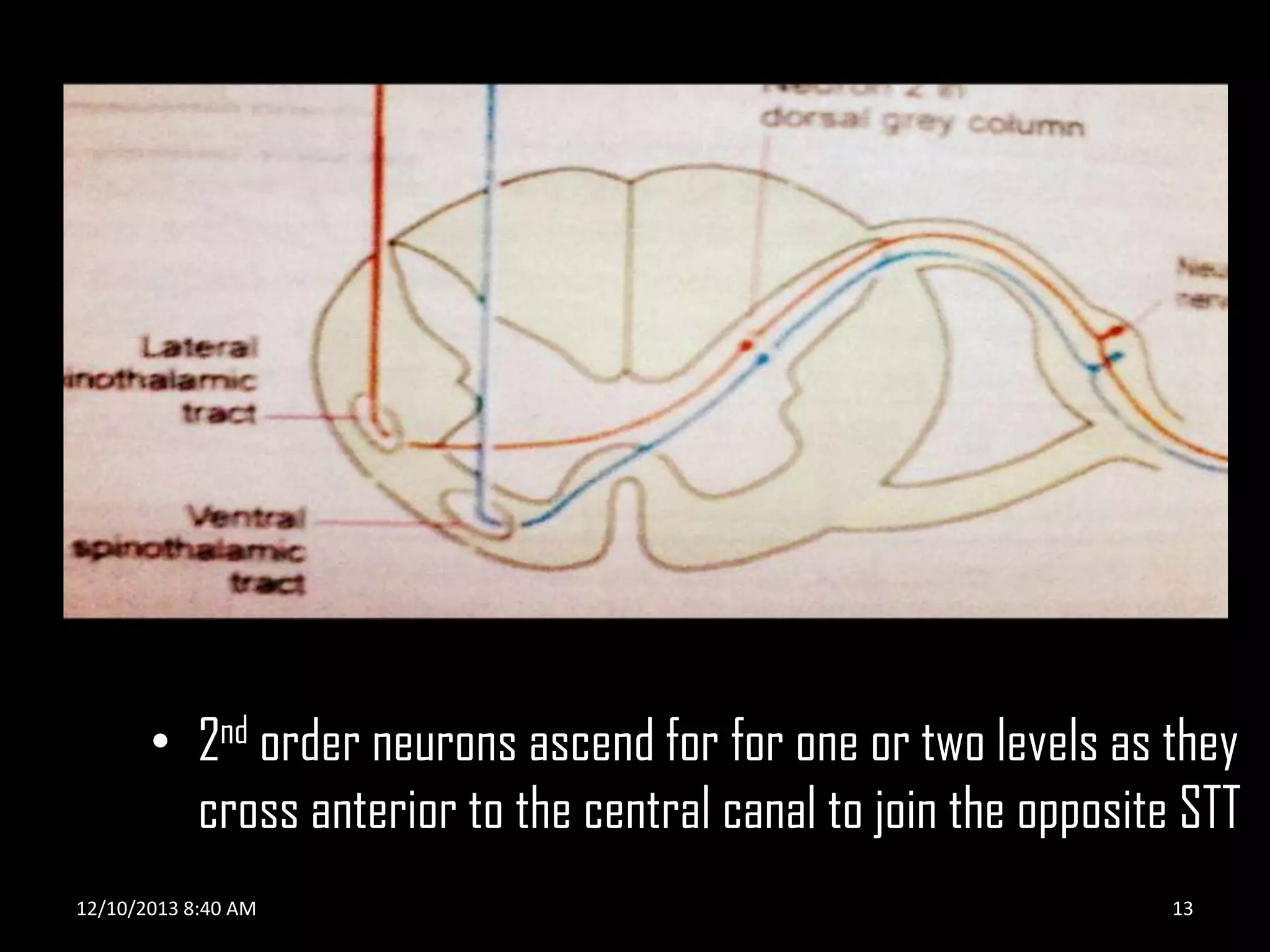
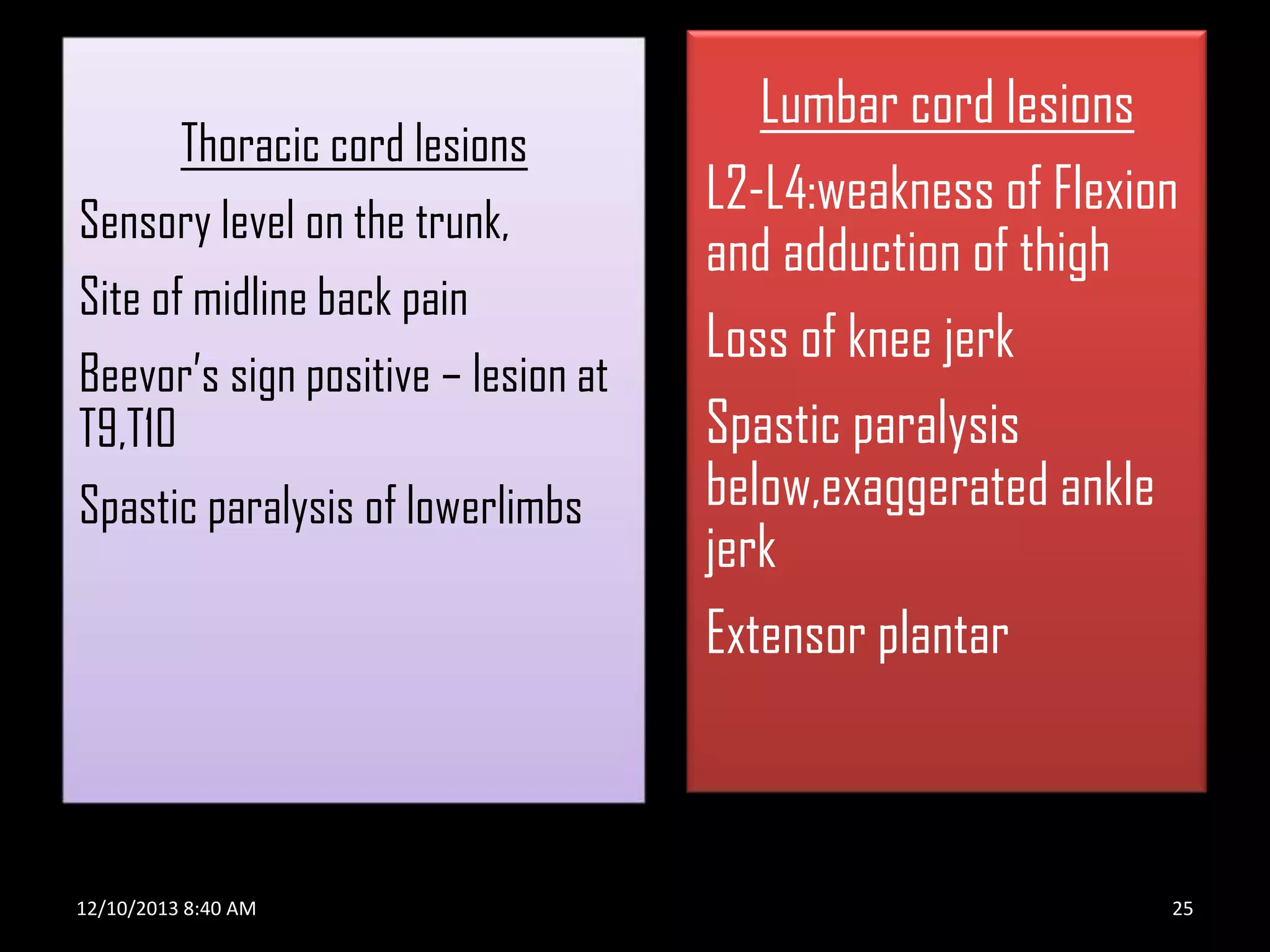
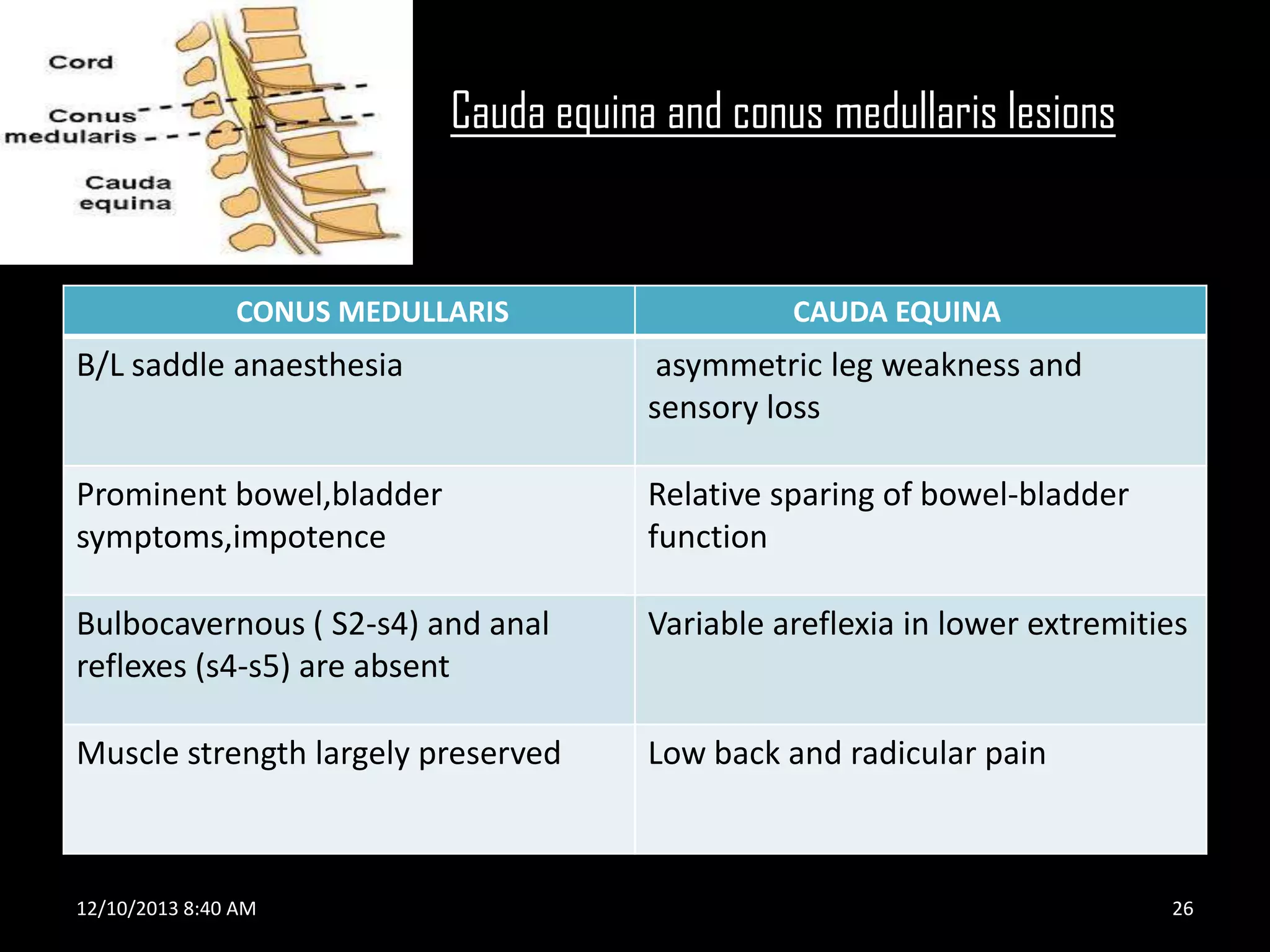
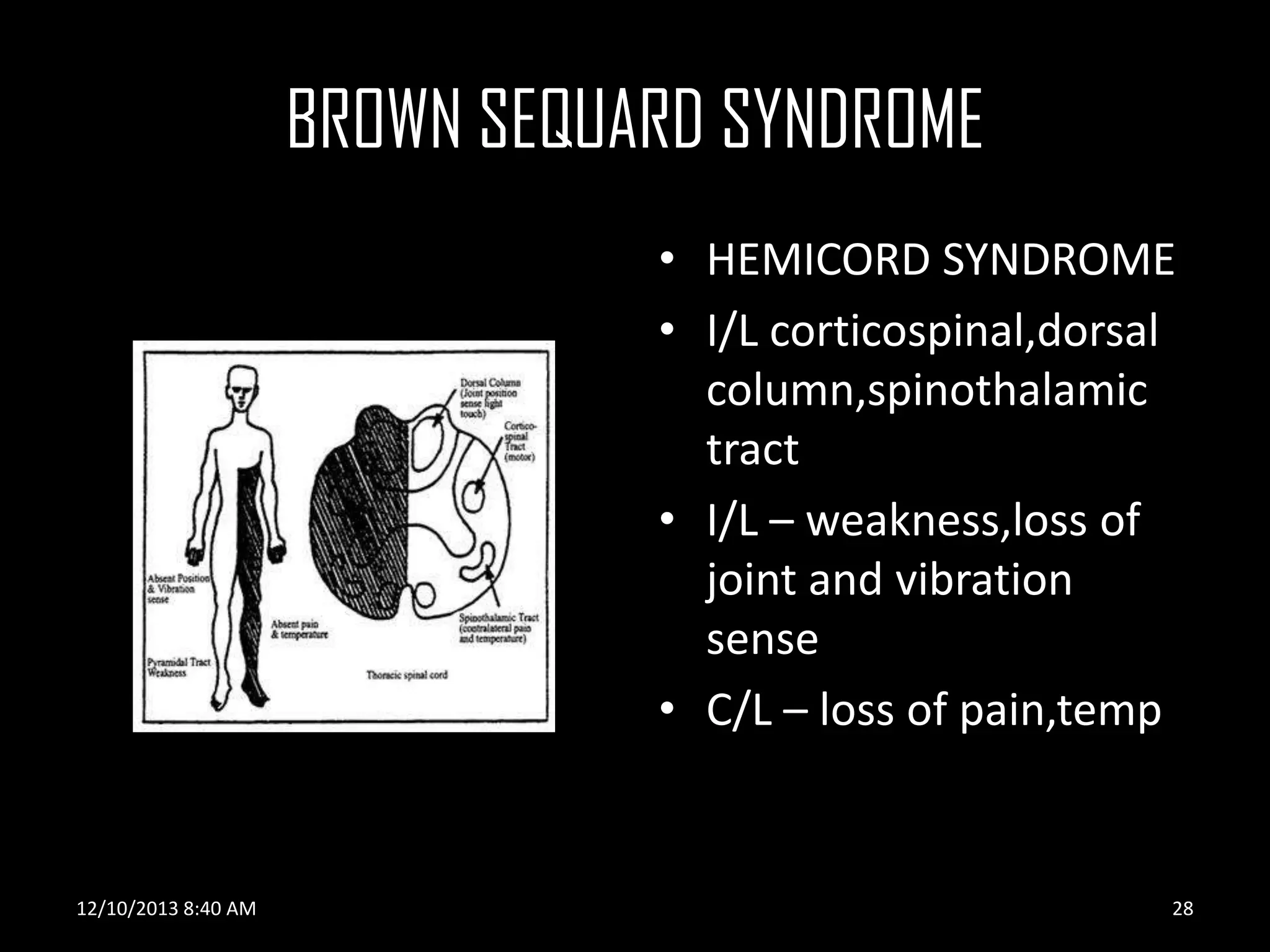
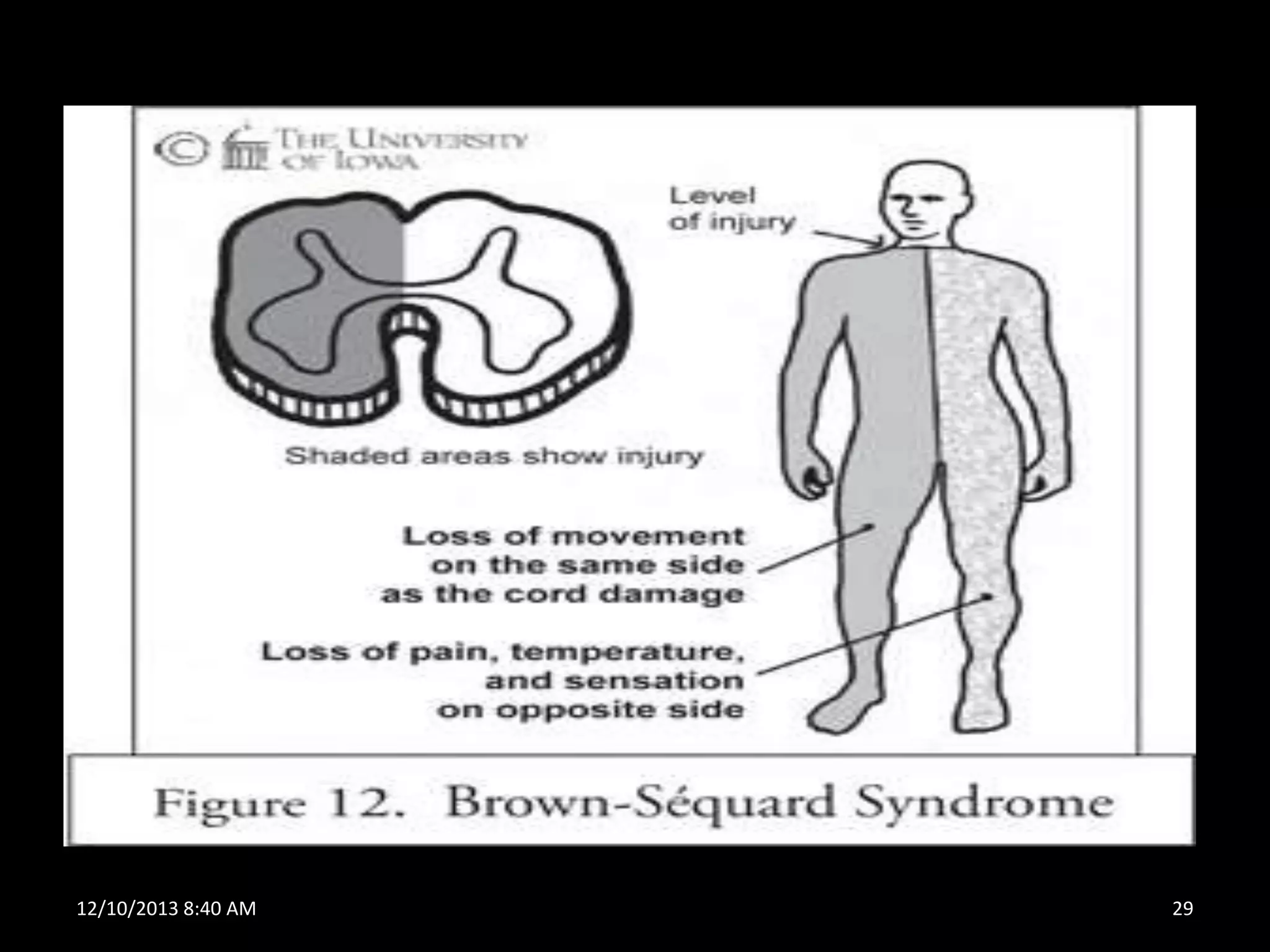
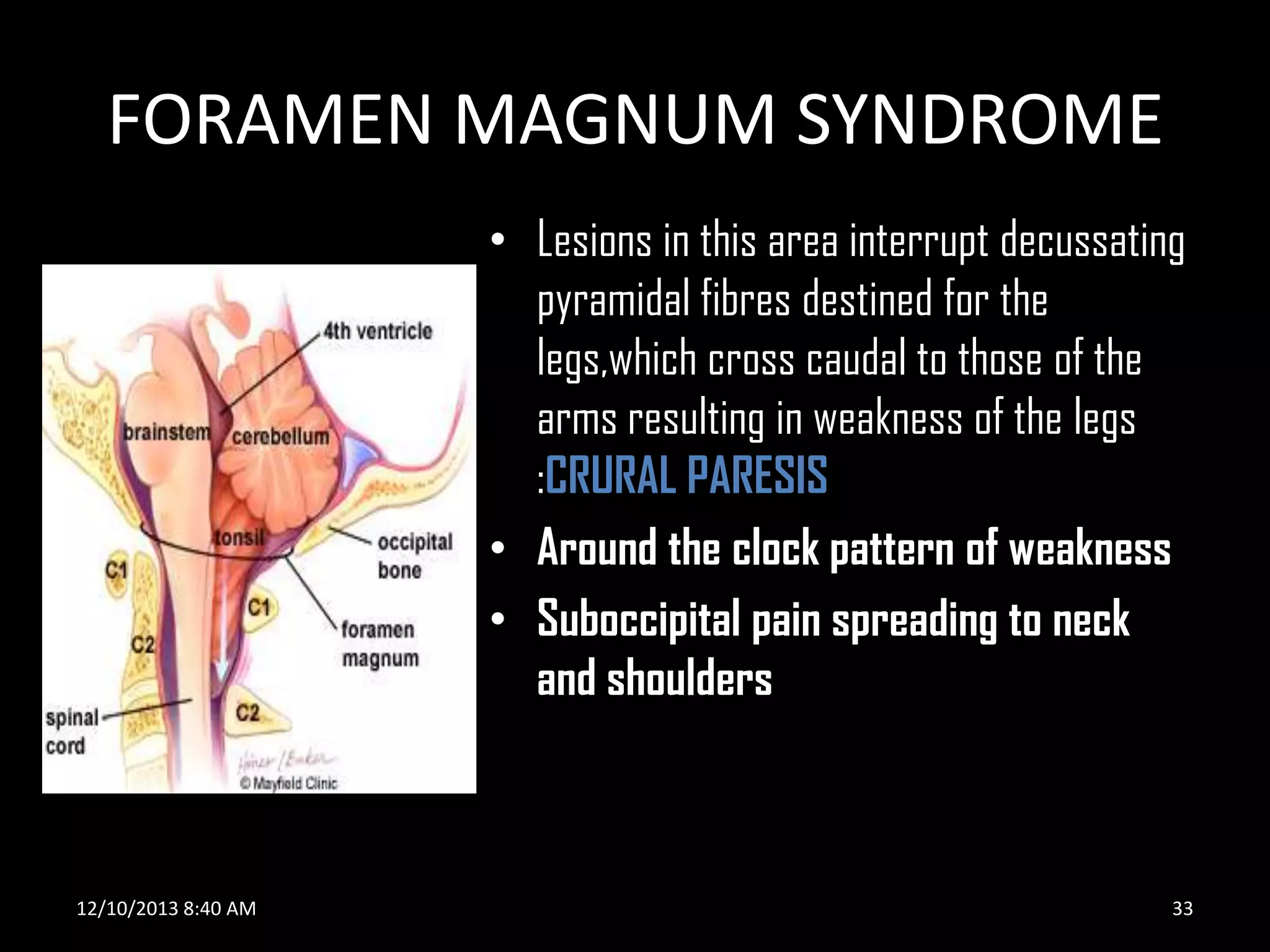
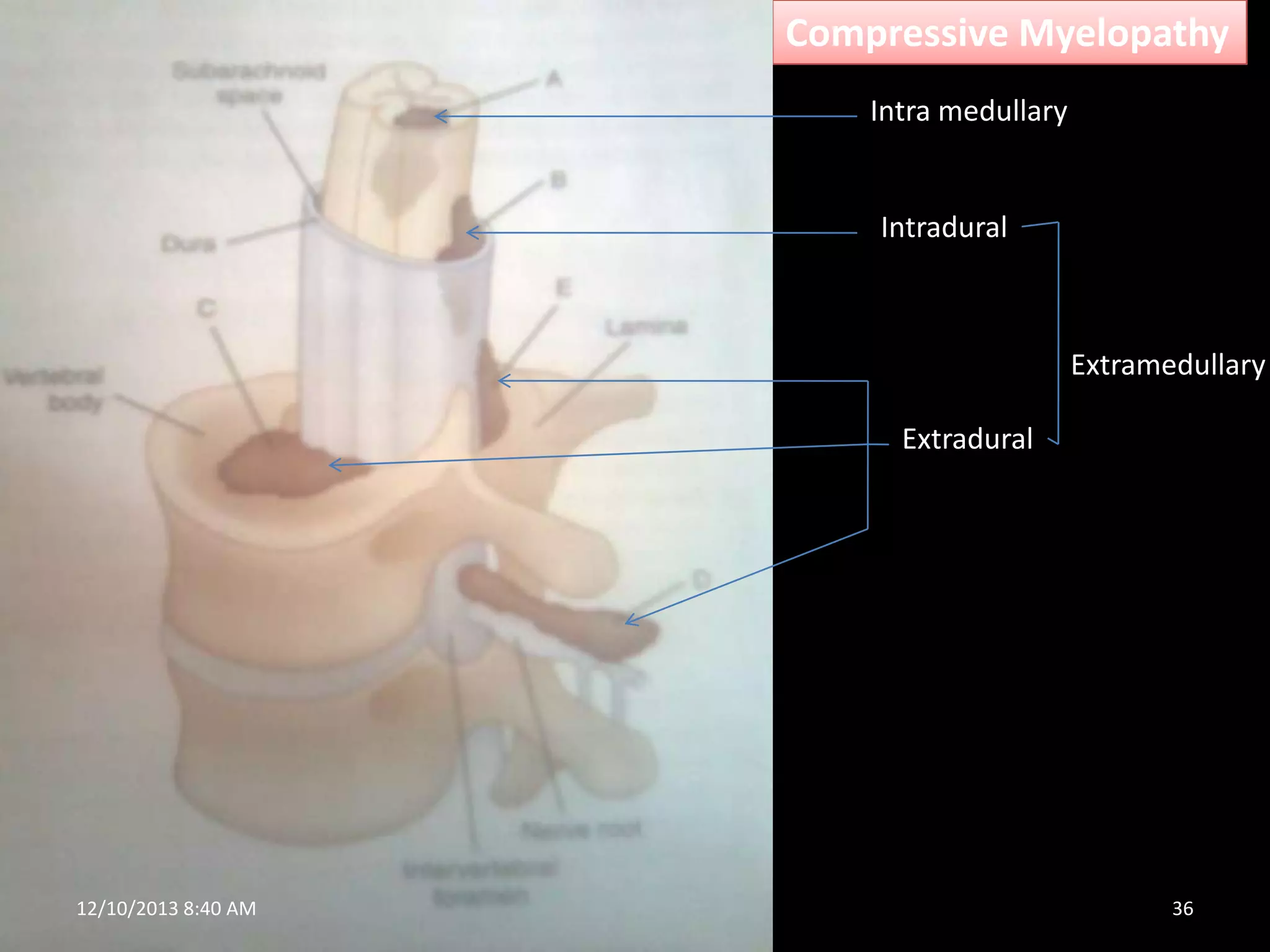
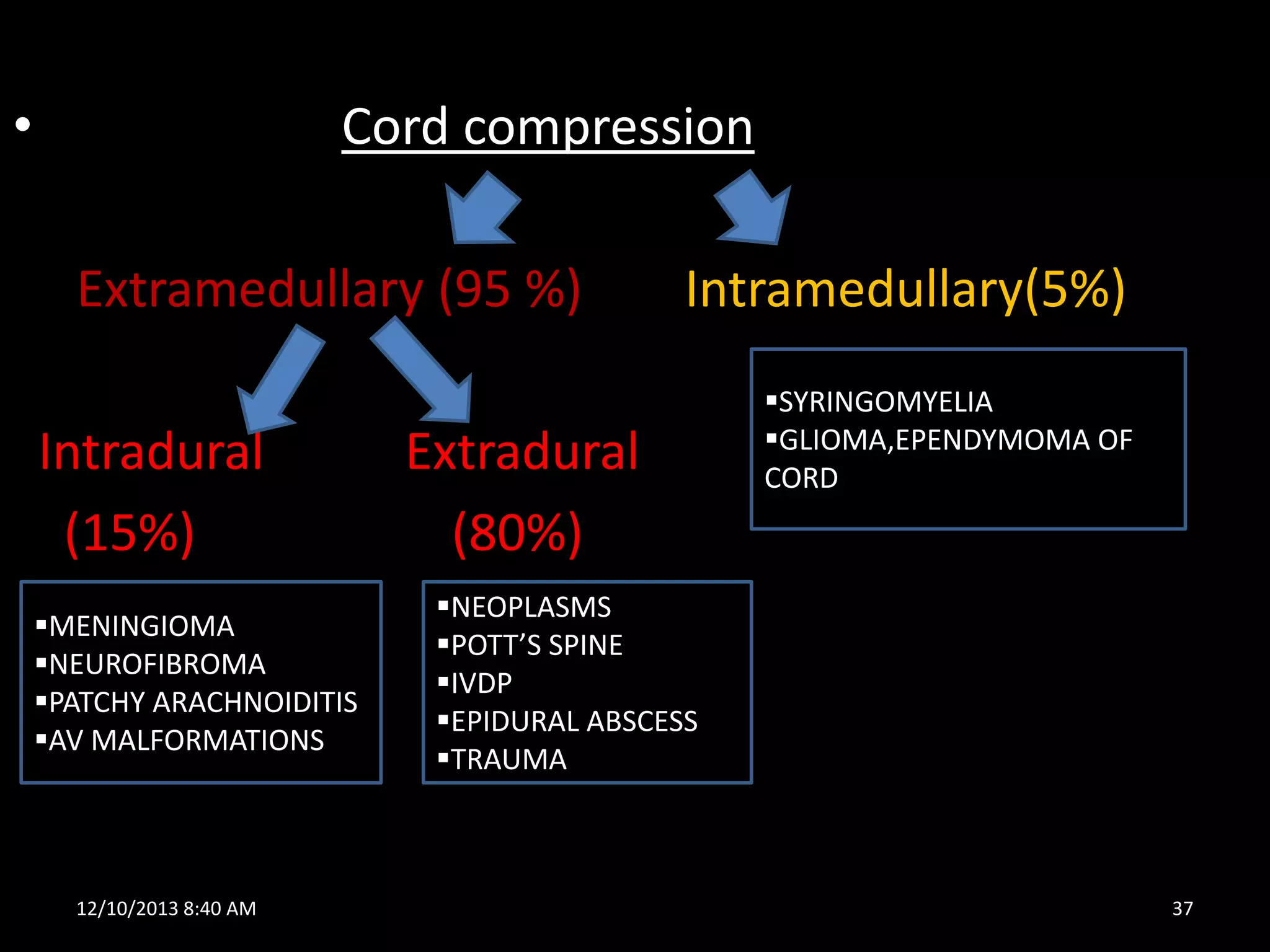


The document discusses the spinal cord and compressive disorders that can affect it. It begins with the basics of spinal cord anatomy and concepts for determining the level of a spinal cord lesion. It then covers special patterns of spinal cord diseases like Brown-Sequard Syndrome. The majority of the document focuses on the different causes of compressive myelopathy, distinguishing between intramedullary and extramedullary lesions, as well as intradural and extradural causes. Common extradural compressive disorders discussed include intervertebral disc prolapse, spinal epidural abscess, and spinal tumors.



































































