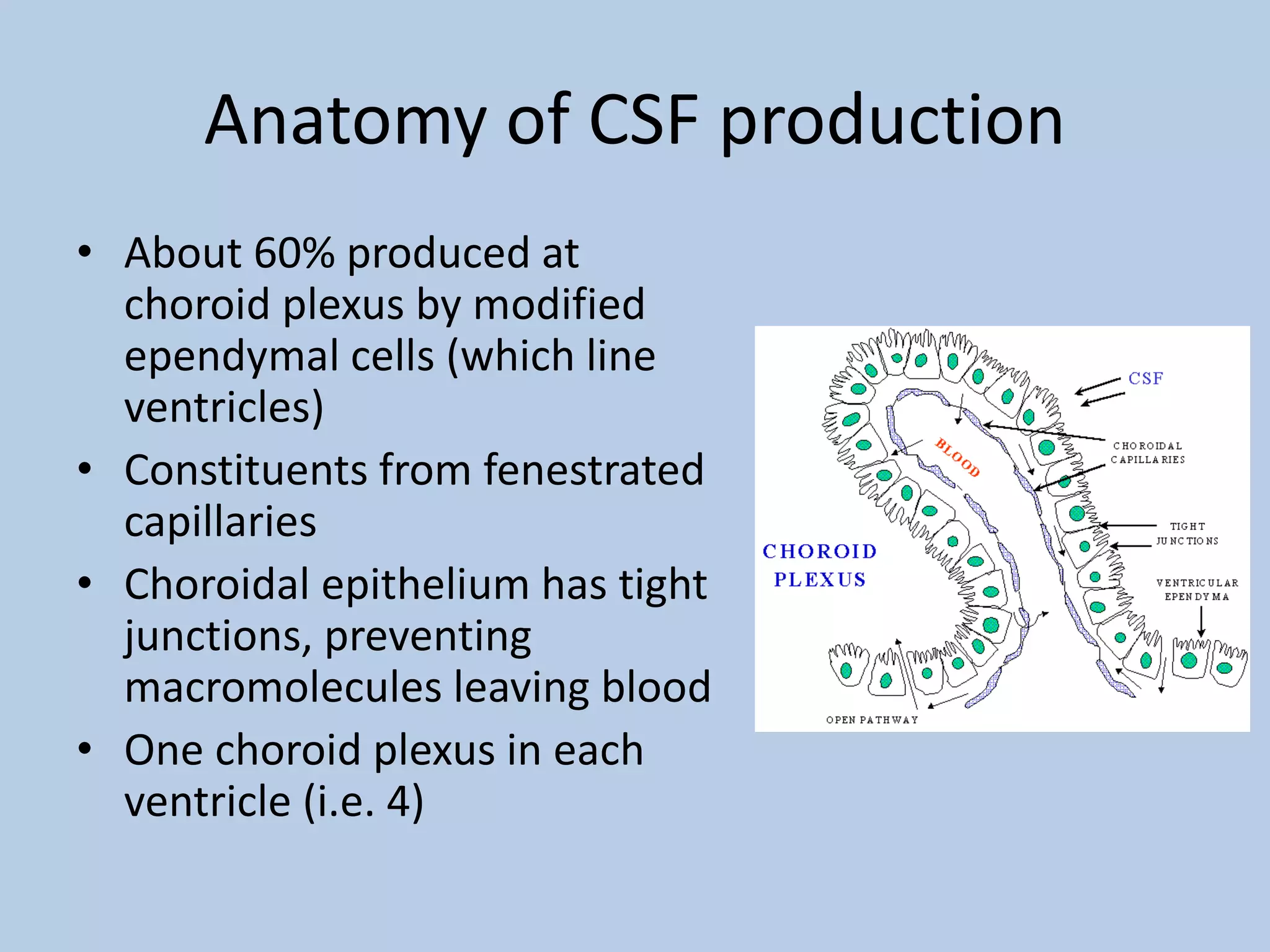
This document provides information about cerebrospinal fluid (CSF) and interpreting lumbar puncture results. It discusses how CSF is produced and circulated in the brain and spinal cord. Key functions of CSF include preventing ischemia, maintaining chemical stability, protecting the brain, and providing buoyancy. The document outlines normal CSF constituents and indicates when lumbar punctures are used. Abnormal protein, glucose, white blood cell counts, or blood-stained CSF can indicate infections or other conditions.