Downloaded 1,218 times
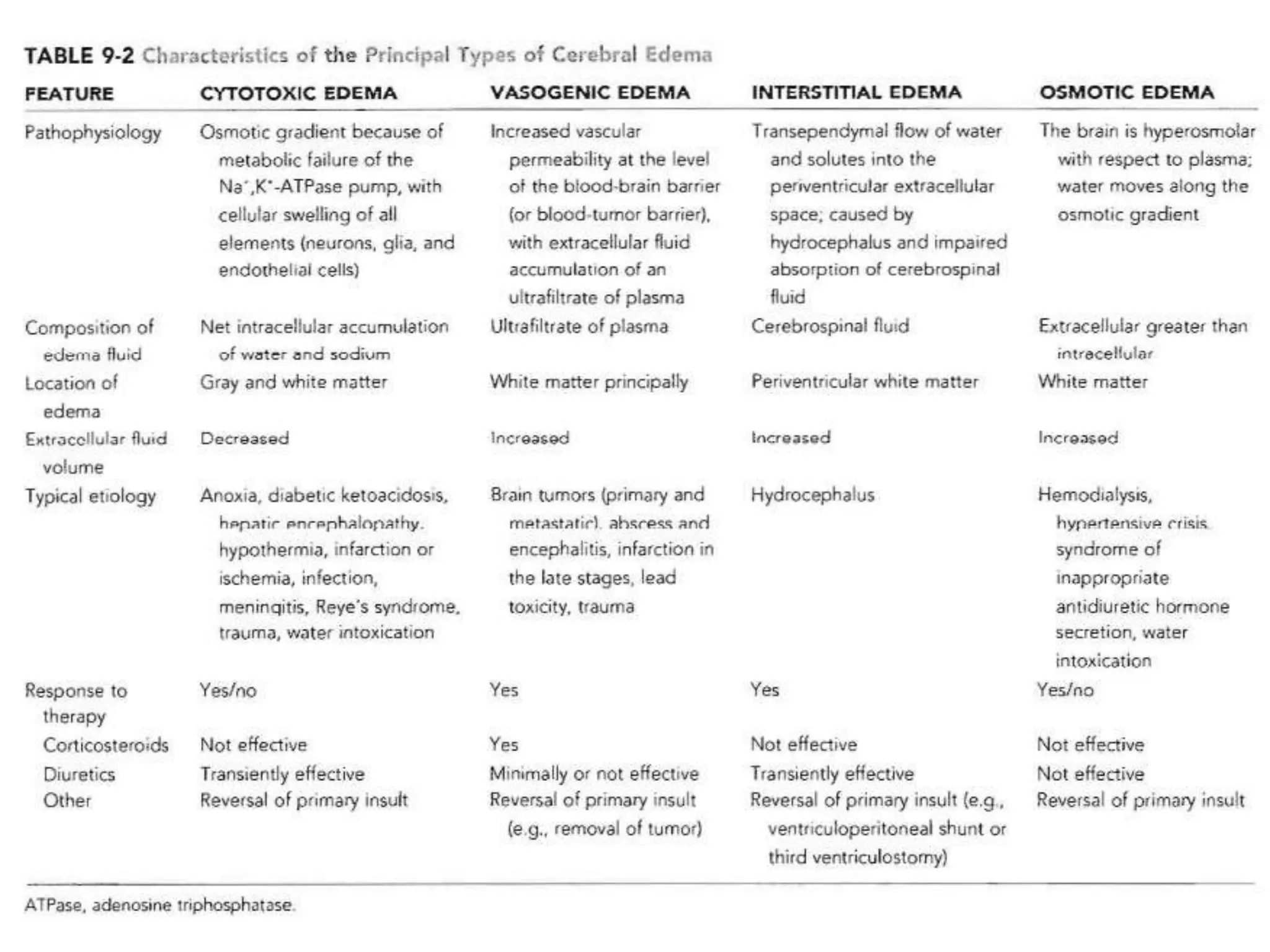

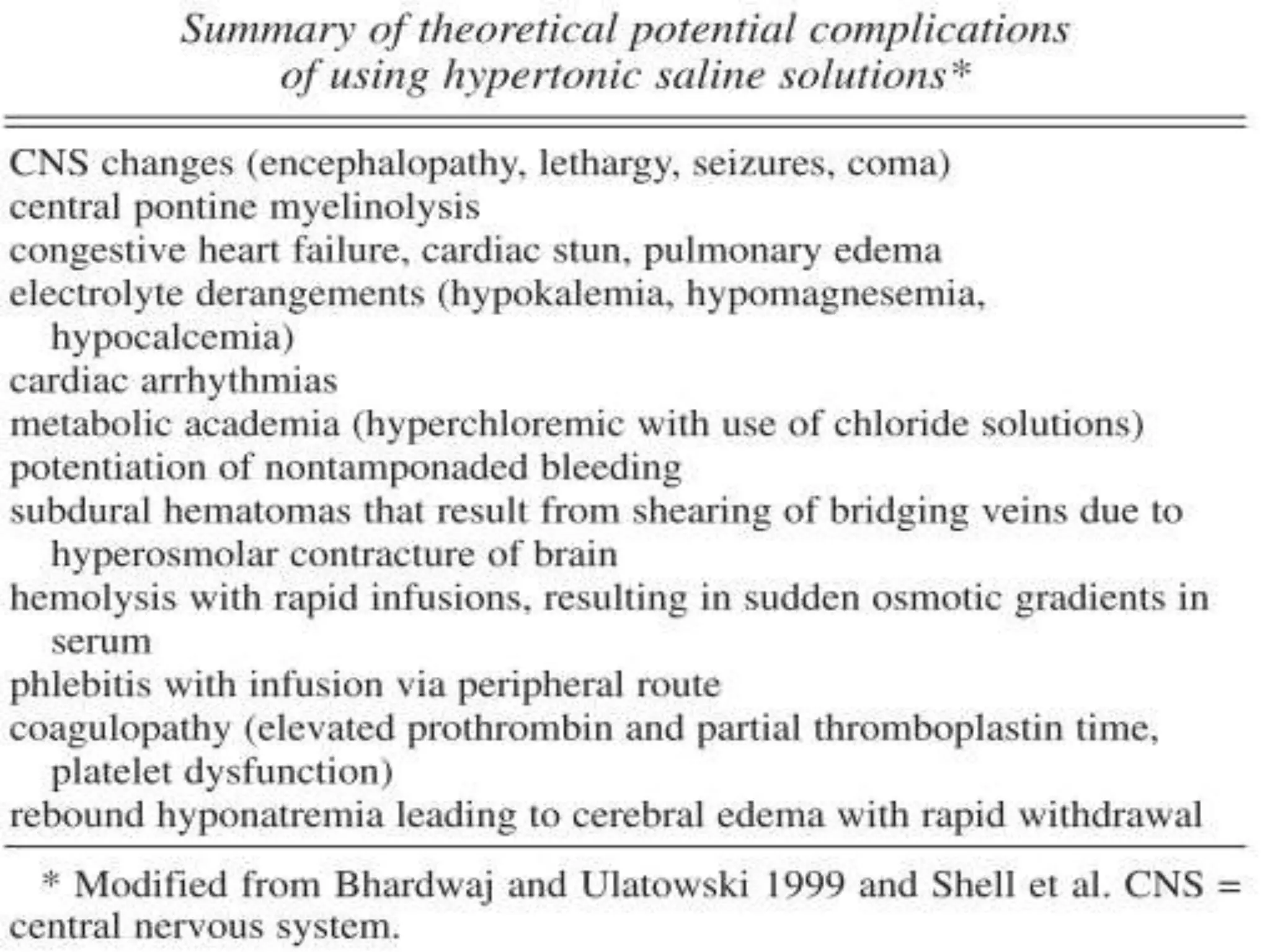


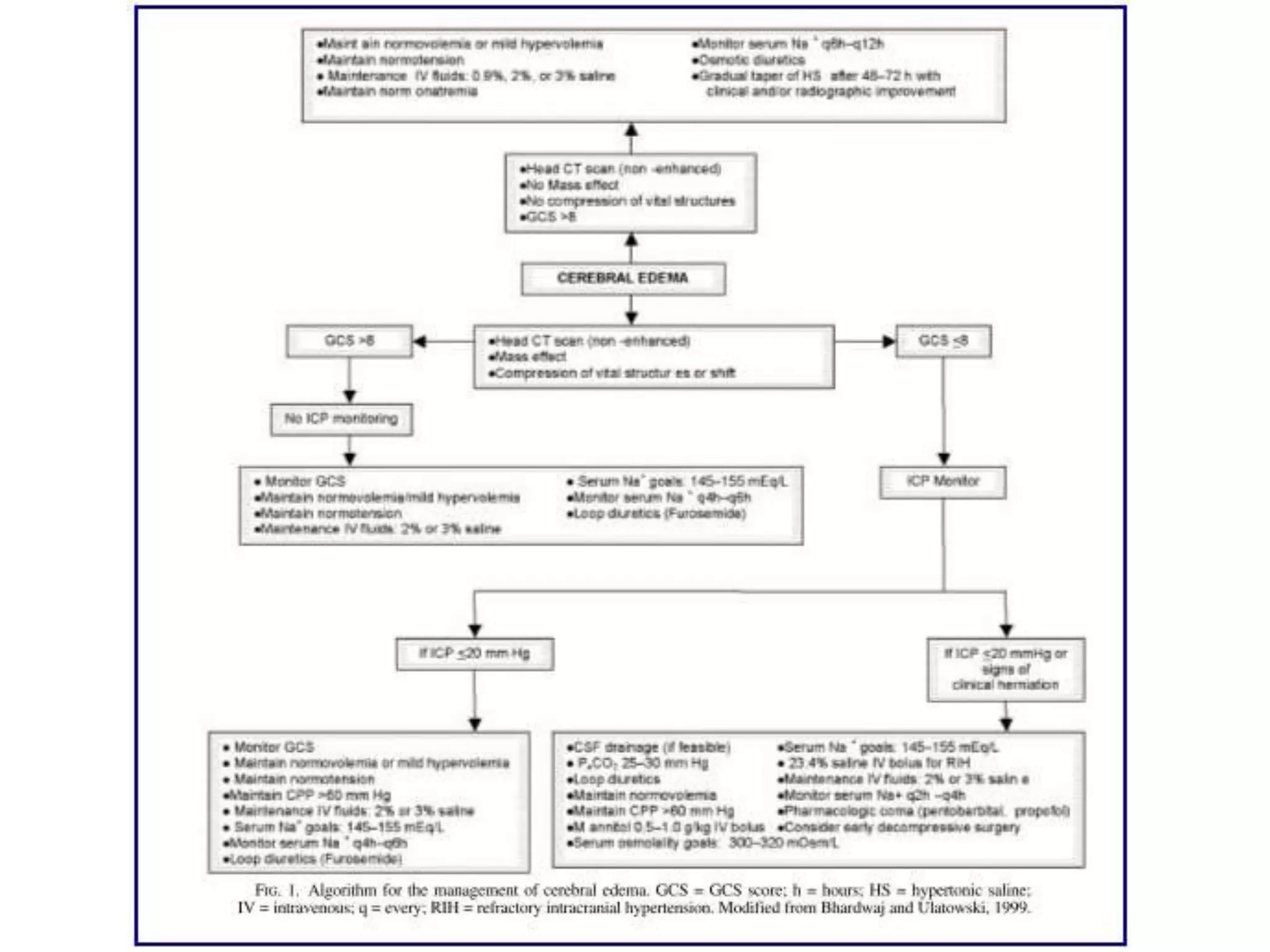
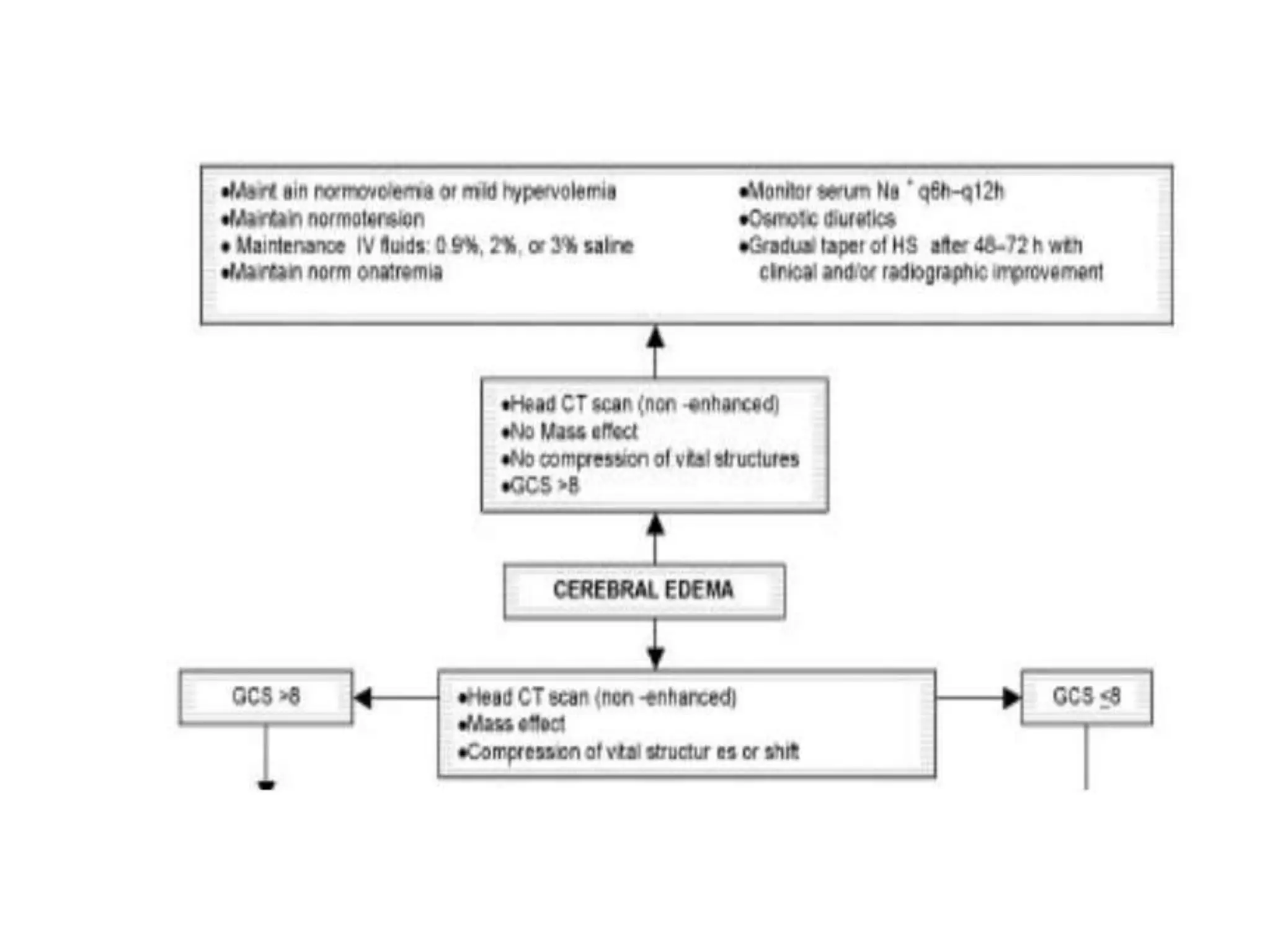
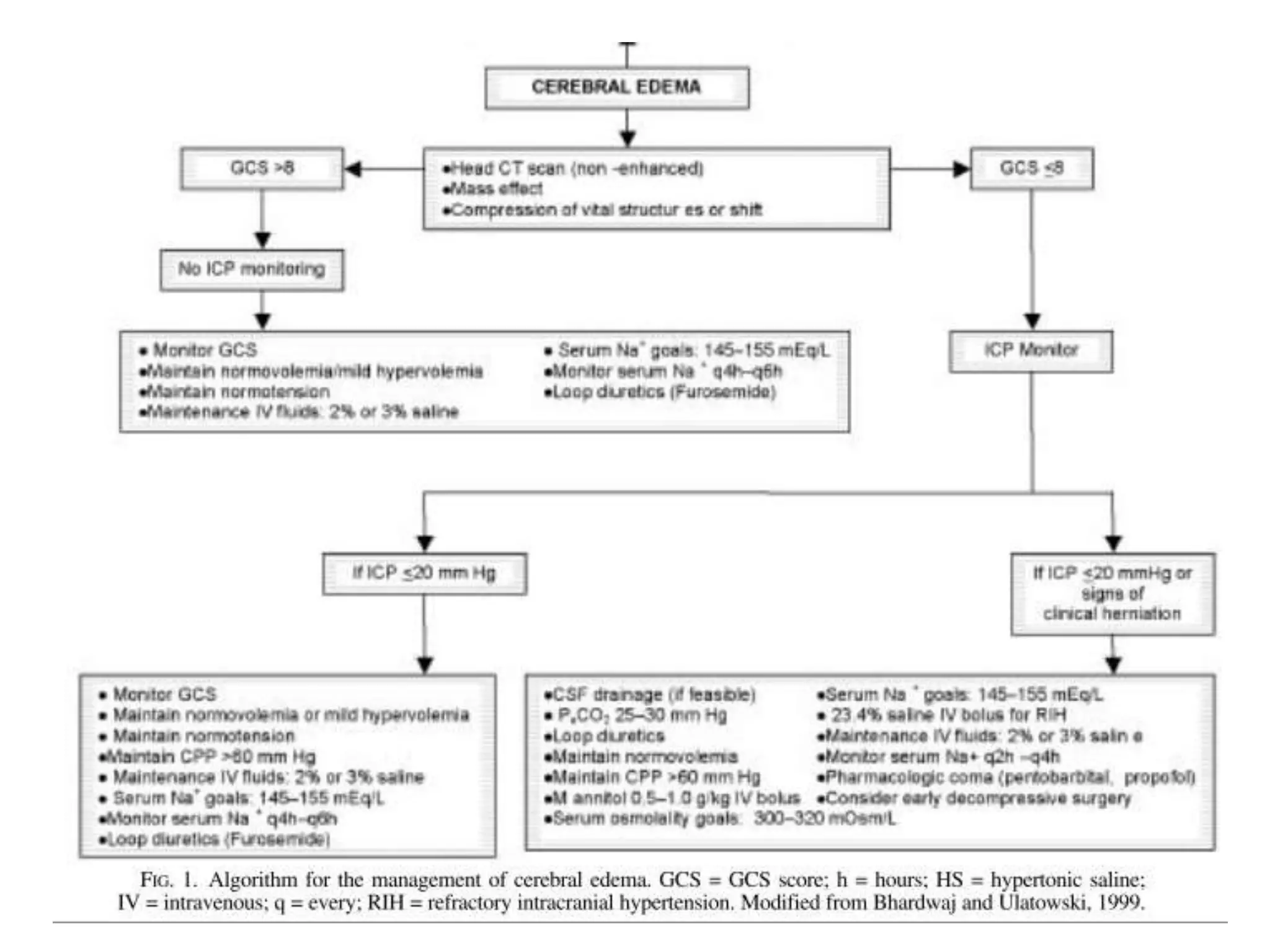

This document discusses different types of cerebral edema including cytotoxic, vasogenic, hydrostatic, osmotic, and hydrocephalic edema. It provides details on the causes, mechanisms, and management of each type. The key management strategies for cerebral edema discussed are head elevation, oxygenation, fluid management, seizure prophylaxis, fever control, nutrition, hyperventilation, osmotherapy using mannitol, and other adjunctive therapies.












































![Management of Cerebral edema 1 [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/managementofcerebraledema1autosaved-231006090123-7bf6a0fb-thumbnail.jpg?width=640&height=640&fit=bounds)



































