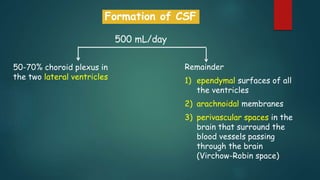
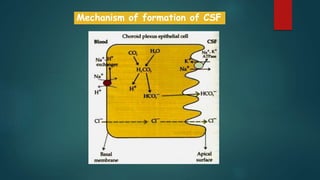
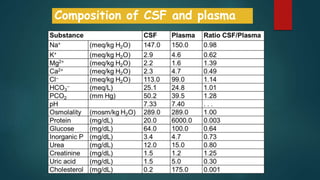
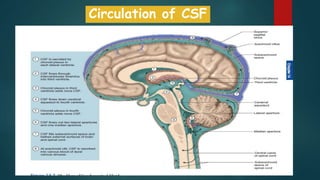
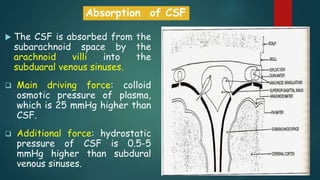
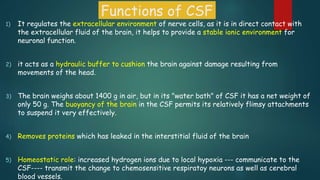
The document discusses the formation, circulation, and functions of cerebrospinal fluid (CSF) and the structure and functions of the blood-brain barrier (BBB). CSF is produced daily by the choroid plexus and plays key roles in maintaining the brain's ionic environment, providing cushioning, and facilitating waste removal. The BBB protects the brain from toxins and regulates substance exchange, but poses challenges for drug delivery in treating brain diseases.