Downloaded 208 times
![DEFINITION OF STROKE
Cerebral vascular accident has been defined as ‘a
sudden, non-convulsive loss of neurologic function due to
an ischemic or hemorrhagic intracranial vascular event’
(pubmed [medline], mesh database, 2005).
The world health organization (who) definition of stroke is:
“rapidly developing clinical signs of focal (or global)
disturbance of cerebral function, with symptoms lasting 24
hours or longer or leading to death, with no apparent cause
other than of vascular origin”](https://image.slidesharecdn.com/stroke-140409032138-phpapp02/85/Stroke-2-320.jpg)



![ Robotics has been defined as: ‘The application of electronic,
computerized control systems to mechanical devices
designed to perform human functions’. (PubMed [Medline],
MeSH database, 2005).](https://image.slidesharecdn.com/stroke-140409032138-phpapp02/85/Stroke-56-320.jpg)
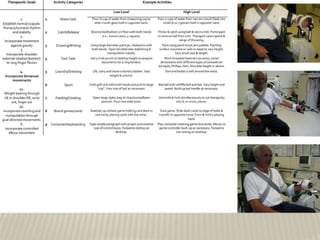

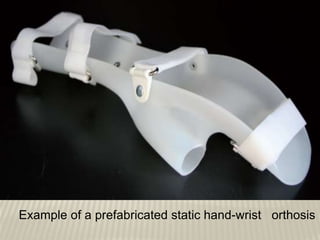
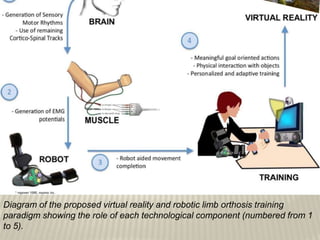
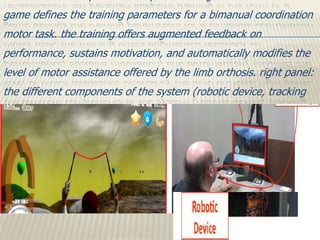
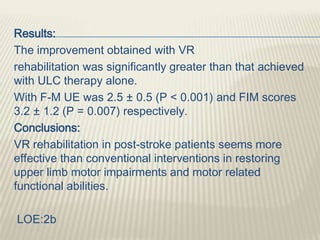
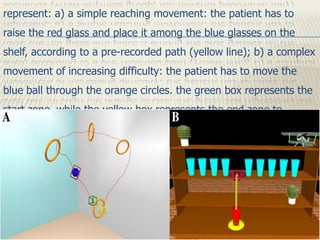
The document discusses recent advances in managing upper limb impairments after stroke. It describes studies that evaluated the long-term use of static hand-wrist orthoses, the use of table-top exergames to improve arm function, and a pilot study combining virtual reality and a myoelectric limb orthosis to restore movement. It also summarizes a controlled trial finding that non-immersive virtual reality treatment can effectively restore upper limb motor function and impact daily living activities when combined with conventional upper limb therapy.








































































![intriduction to physiology [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/intriductiontophysiologyautosaved-240606012950-2a373321-thumbnail.jpg?width=640&height=640&fit=bounds)
























