Downloaded 42 times
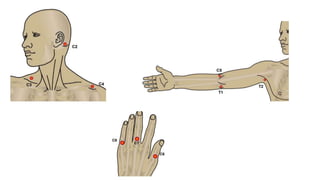
![Sensory examination
• Testing is done bilaterally using Light Touch (LT) and Pin-Prick
(PP) [sharp-dull discrimination].
• Items used:
• a cotton tip
• safety pin
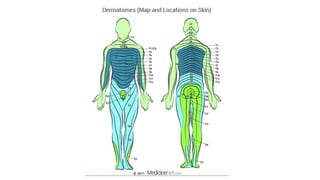
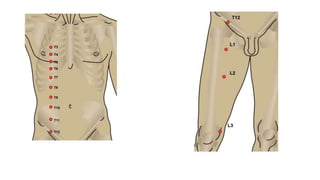
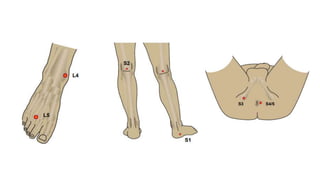
• We follow the dermatomal pattern for sensory assessment. The
sensory key points are used for standardized assessment technique.
• Comparison of the LT is done with the sensation on the patient’s
cheek.](https://image.slidesharecdn.com/asiascale-221002162859-453f85ea/85/ASIA-Scale-pptx-4-320.jpg)
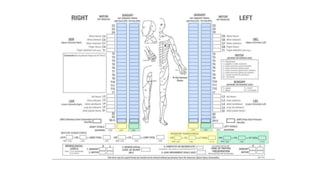
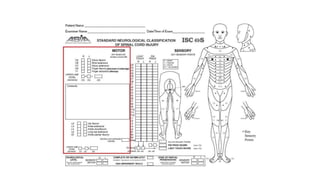
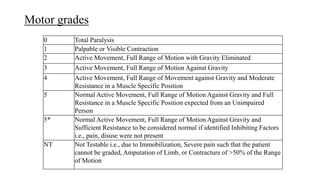
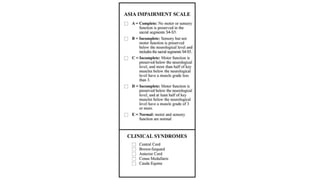

The document outlines the International Standards for Neurological Classification of Spinal Cord Injury (ISNCSCI), detailing standardized examination methods for assessing motor and sensory function loss following spinal cord injuries. It describes the procedures for sensory and motor examinations, including the grading system for motor function, and how to determine the neurological level of injury. Additionally, it includes important definitions related to completeness of injury and references to relevant rehabilitation and assessment resources.























































































