
![Types
1. Short term:
Change of FHR from one beat to the next
[Time between cardiac systoles]
in internal fetal scalp electrode
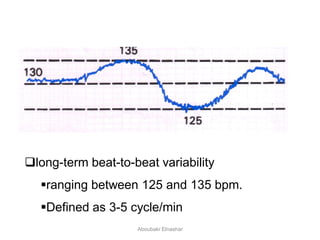
2. Long term:
Oscillation of FHR around baseline /min
[2-6 cycles or waves/min]
Aboubakr Elnashar](https://image.slidesharecdn.com/ctgpatterns-160731155613/85/CTG-patterns-13-320.jpg)
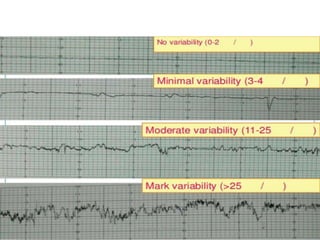
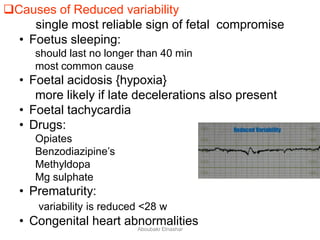
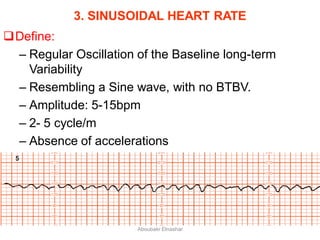
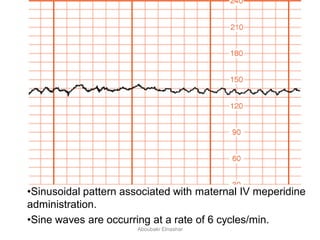
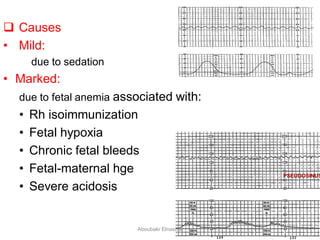
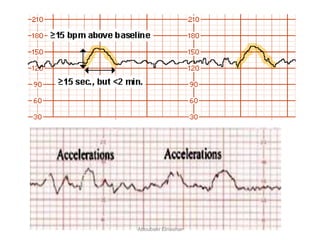
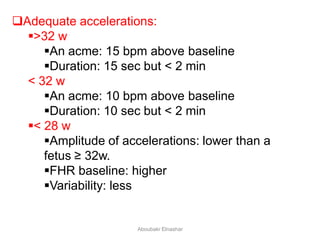
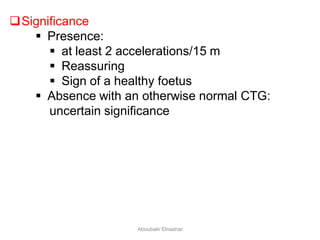
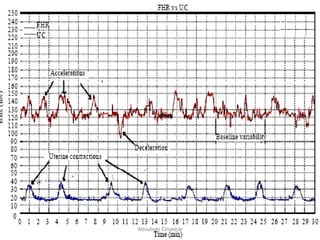
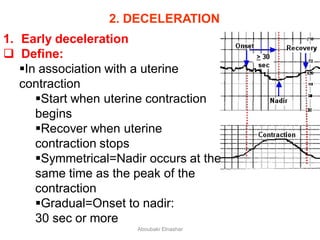
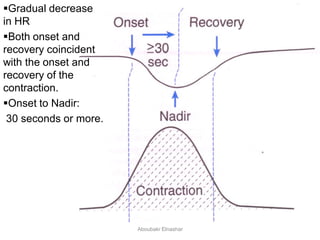
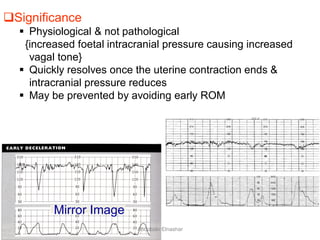
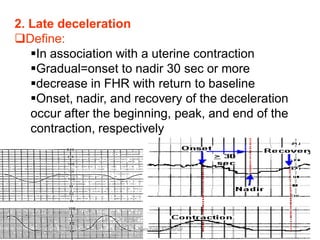
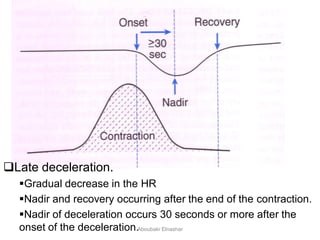
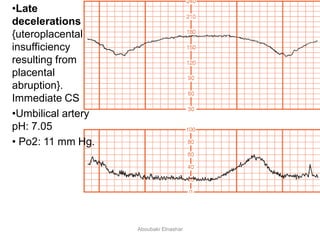
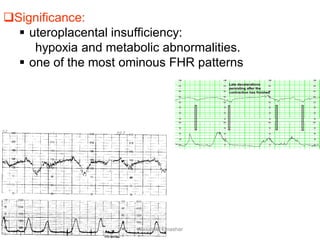
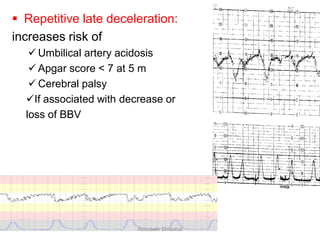
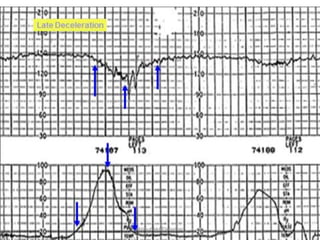
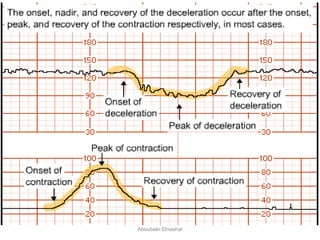

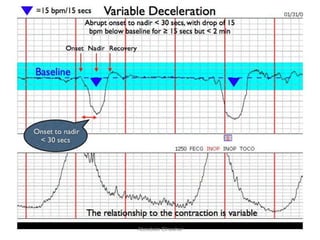
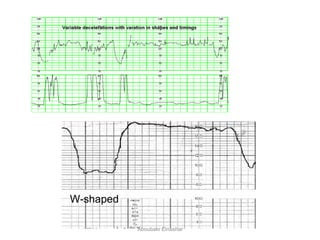
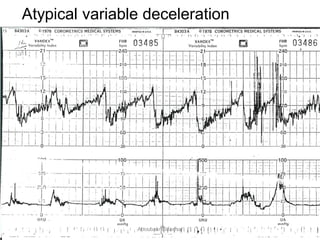
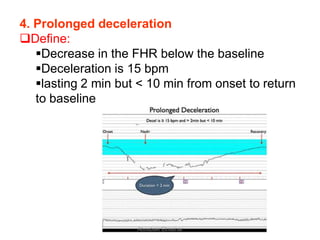
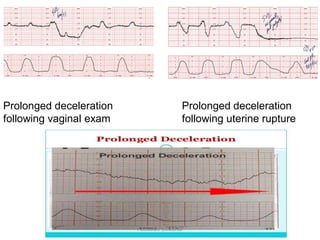
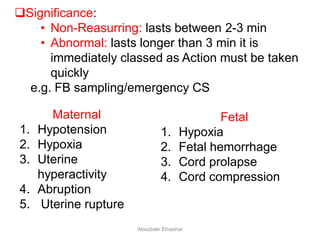
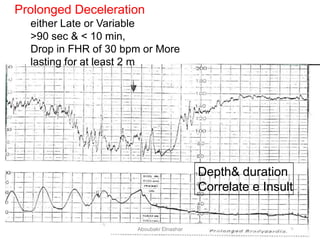
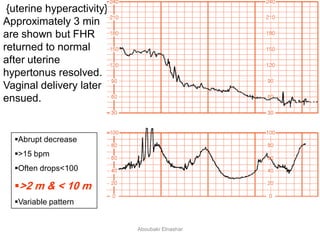
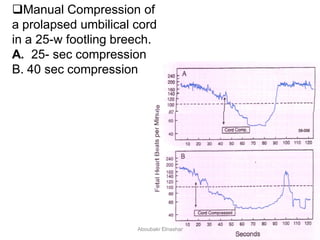
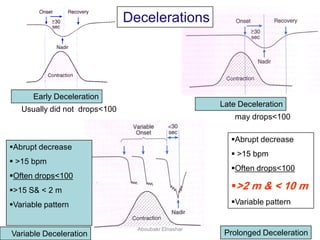


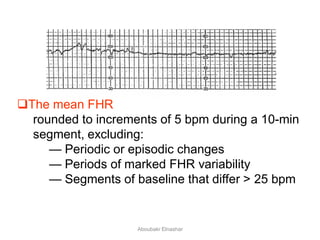
This document discusses various patterns seen on cardiotocography (CTG) monitoring of fetal heart rate. It describes normal baseline heart rate ranges and variability. It also defines different periodic changes seen such as accelerations and decelerations including early decelerations, late decelerations, variable decelerations and prolonged decelerations. Various abnormal patterns are also described such as tachycardia, bradycardia, reduced variability and sinusoidal patterns. Causes and clinical significance of these findings are discussed.



























































![NRFHRP [ Natnael Dechasa ] PPT.pdf](https://cdn.slidesharecdn.com/ss_thumbnails/nrfhrpnatnaeldechasappt-230322120009-fa3db710-thumbnail.jpg?width=640&height=640&fit=bounds)



































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)








![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)


