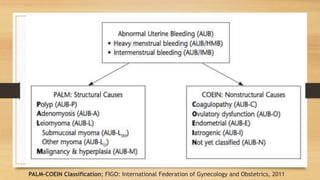
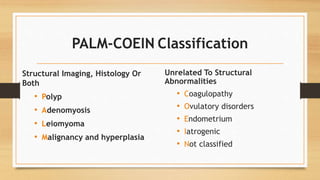
The document discusses abnormal uterine bleeding (AUB), a common issue affecting many women, detailing its classifications, causes, and management strategies. It highlights the importance of understanding the menstrual cycle, normal versus abnormal bleeding patterns, and provides a comprehensive overview of diagnostic approaches and treatment options, including hormonal therapy and surgical interventions. The document also emphasizes a structured assessment and classification system (PALM-COEIN) to standardize terminology surrounding AUB.
































![ABNORMAL_UTERINE[1] DR SS NANda abnormal DA.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/abnormaluterine1drssnanda-250706172120-db732f7a-thumbnail.jpg?width=640&height=640&fit=bounds)











































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)














