



















The document discusses the interpretation and management of CTG (cardiotocography). It describes the steps to interpret a CTG tracing, including evaluating the fetal heart rate baseline, variability, accelerations, decelerations and their correlation with uterine contractions. It provides a structured DR C BRA VADO method to categorize CTG tracings as normal, suspicious or pathological. The management strategies for each category are then outlined, such as continued monitoring, additional tests like fetal scalp blood pH, or expedited delivery depending on the severity of the CTG abnormalities. Specific situations like the second stage of labor, placental abruption or fetal abnormalities are also addressed.
Introduction to CTG interpretation steps including FHR assessments, contraction evaluations, and overall clinical conclusions.
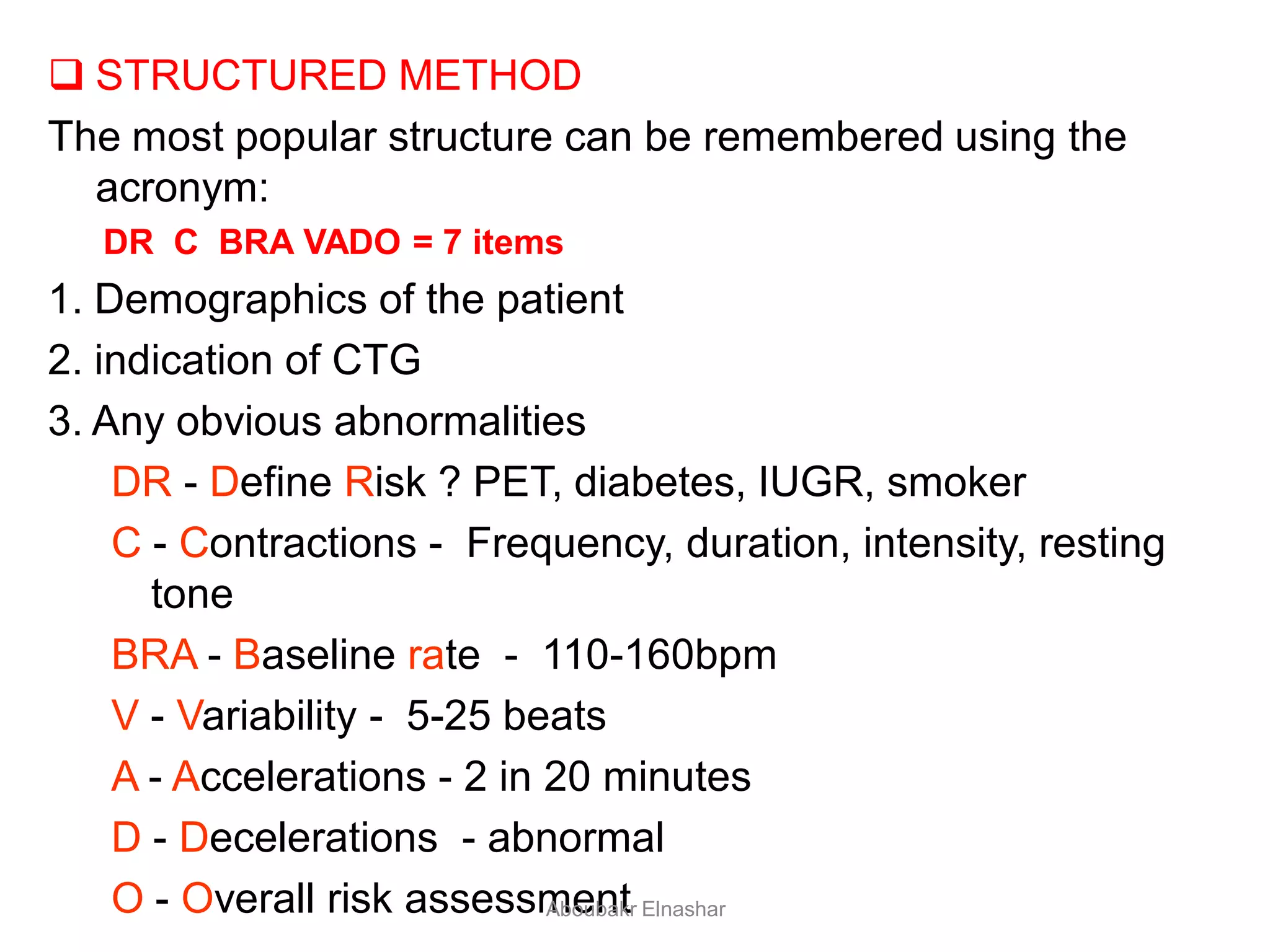
Description of a structured approach (DR C BRA VADO) for evaluating CTG, including risk assessment and overall impressions.
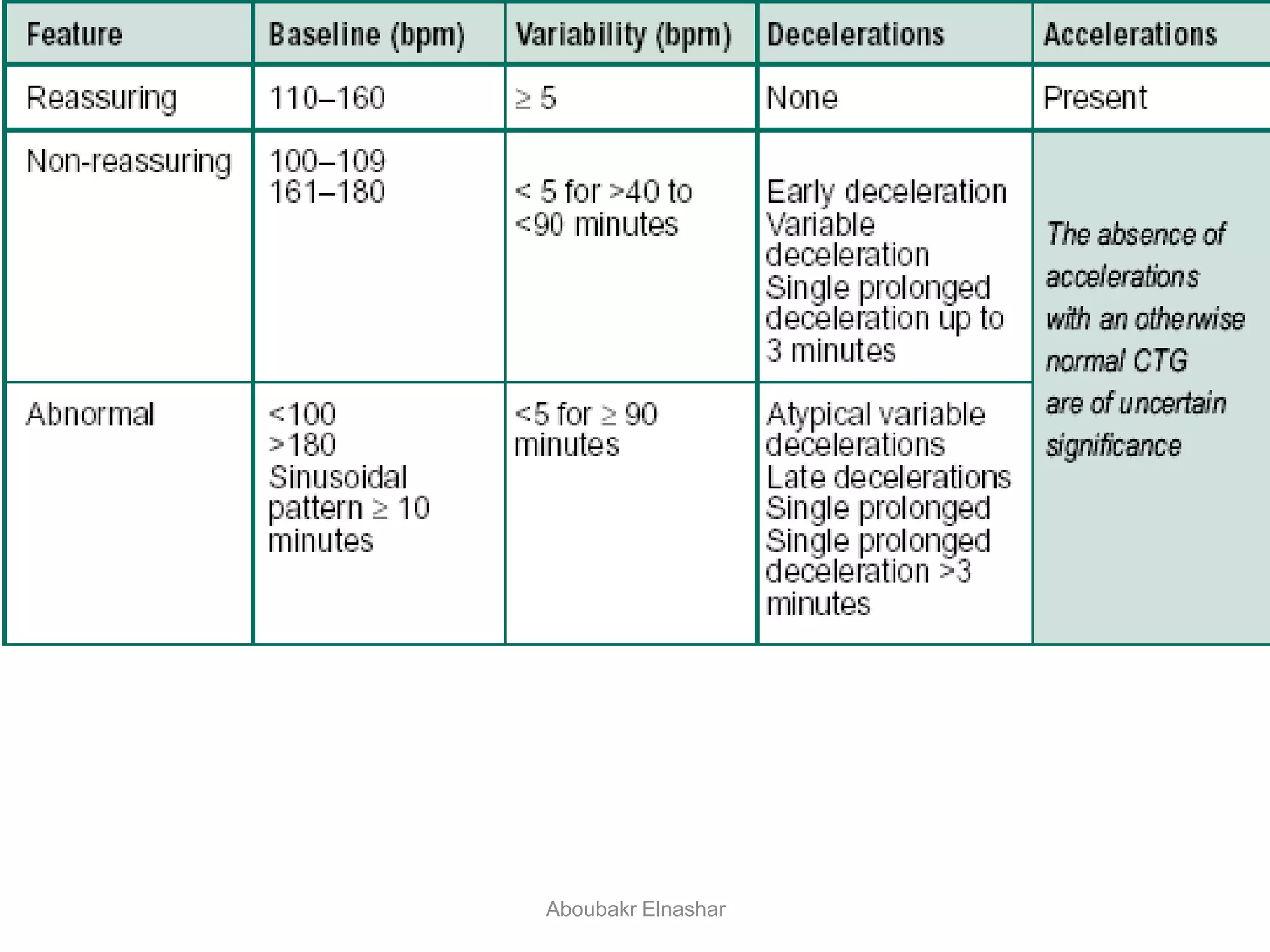
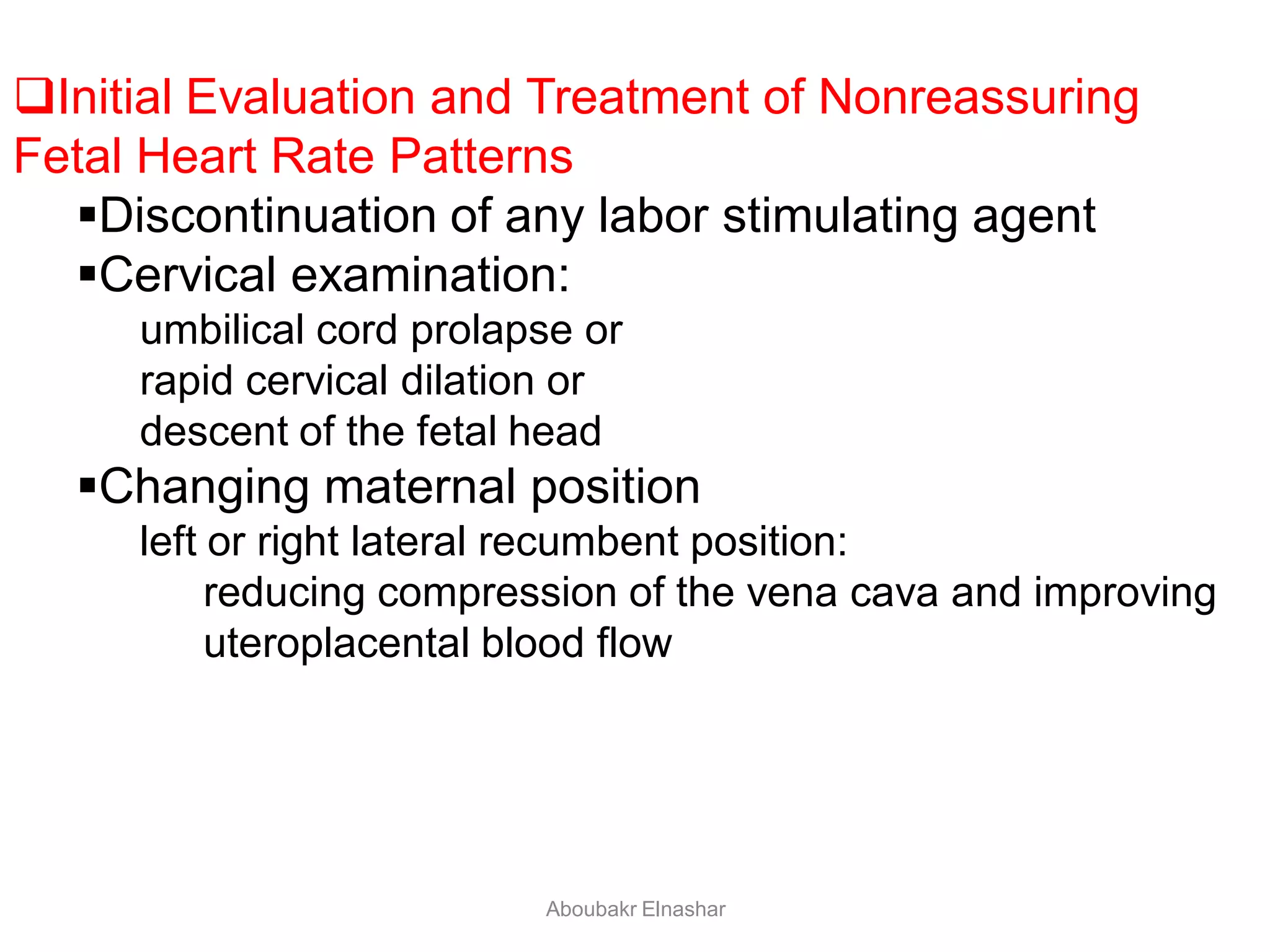
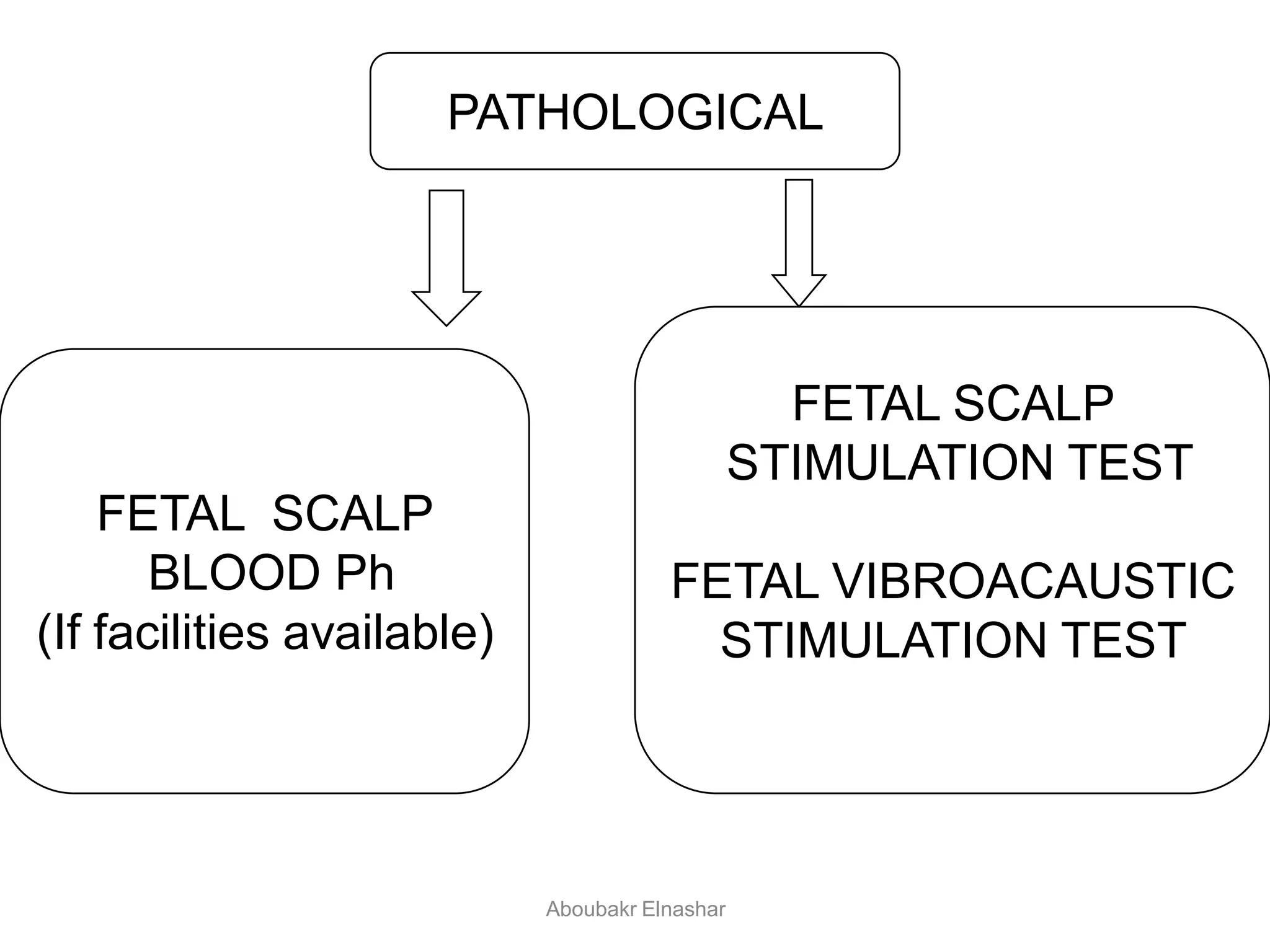
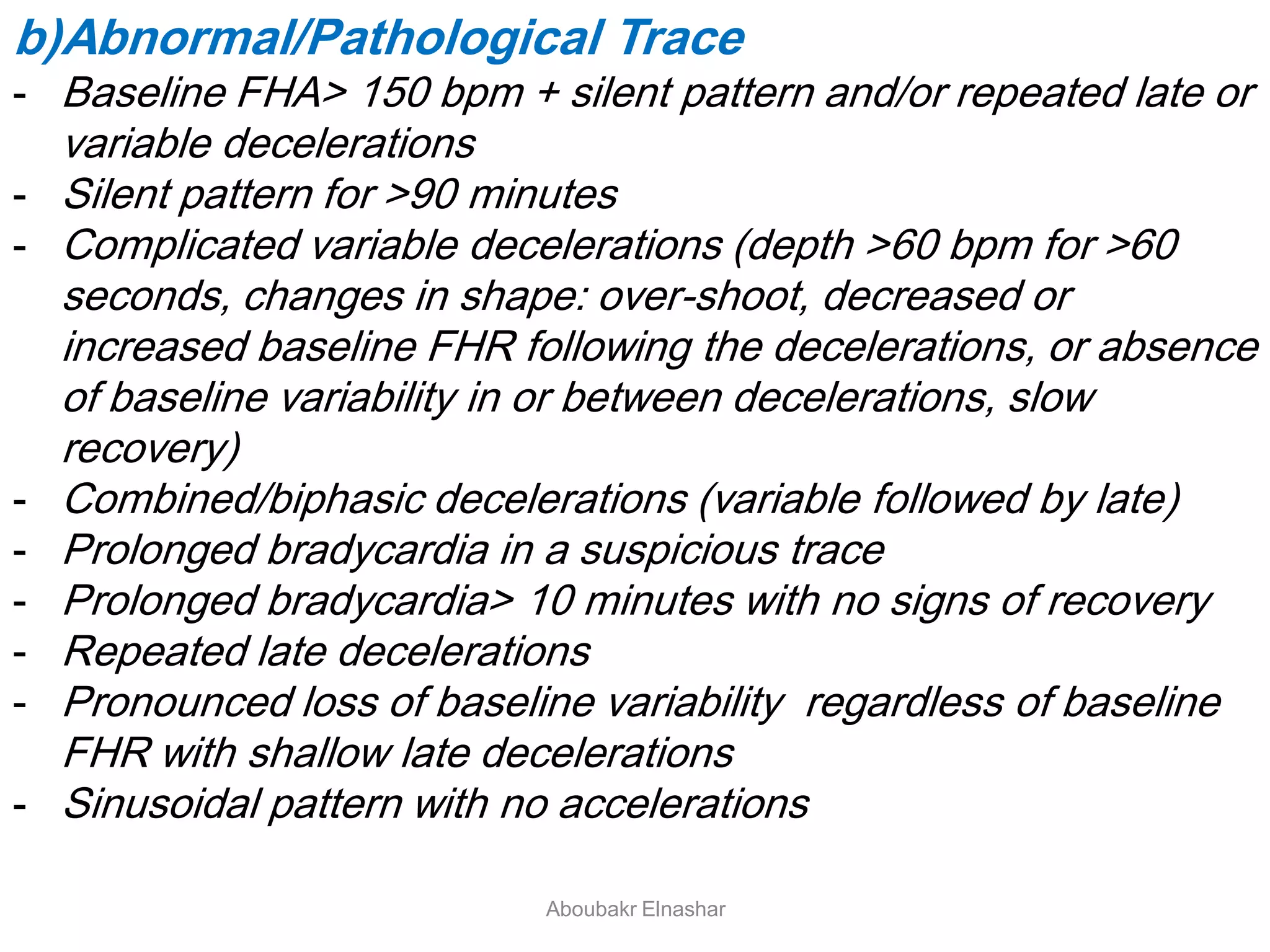
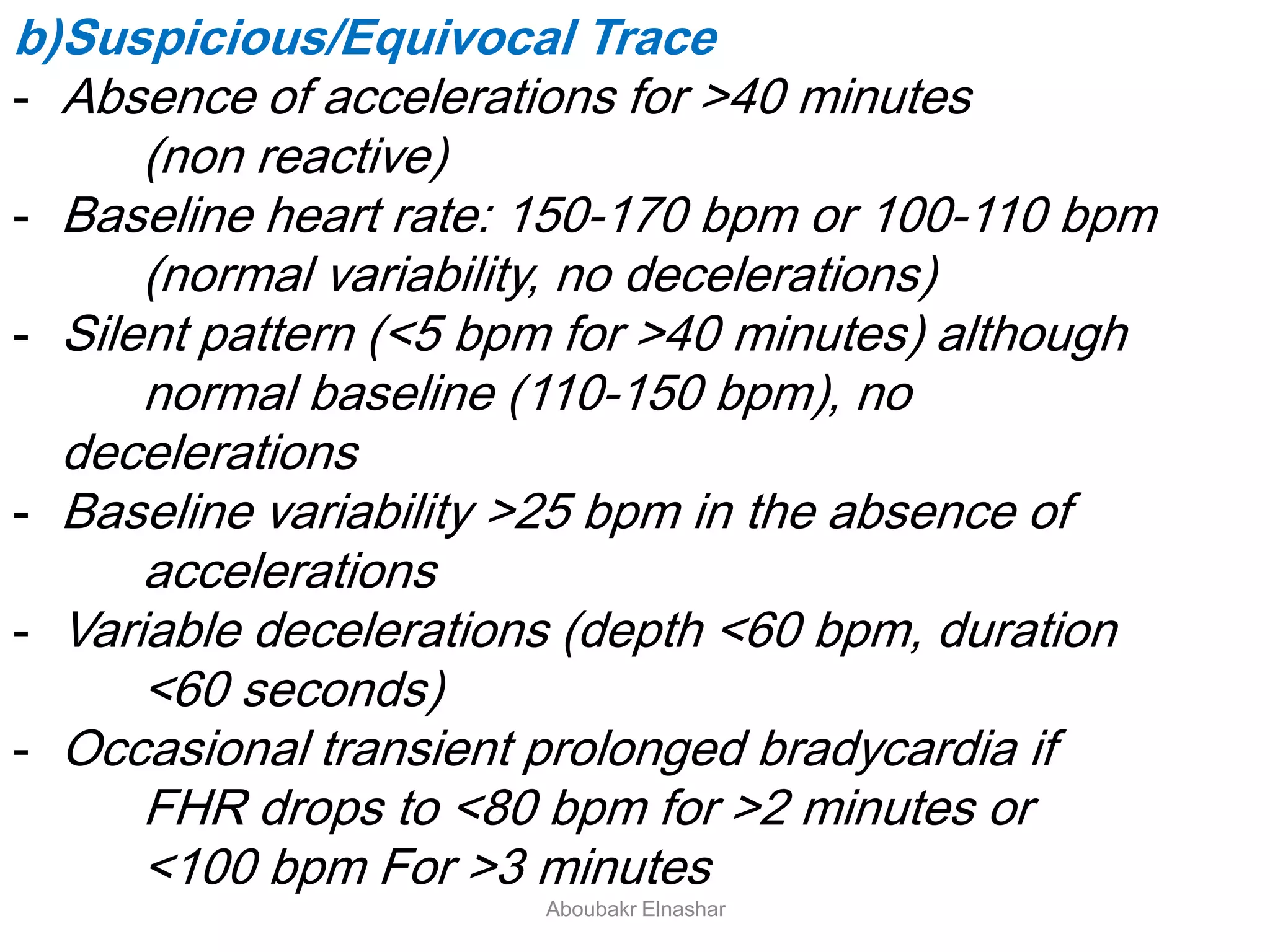
Classification of fetal heart rate patterns (normal, suspicious, pathological) and corresponding management strategies.Assessment of hypoxia signs, placental issues, fetal abnormalities, and heart block indications during labor.
Clinical management strategies for different CTG patterns, detailing normal, suspicious, and pathological classifications.











































































































