Downloaded 265 times
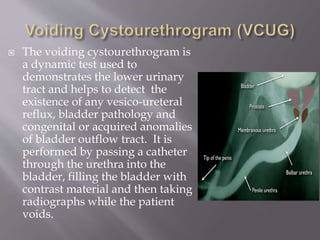
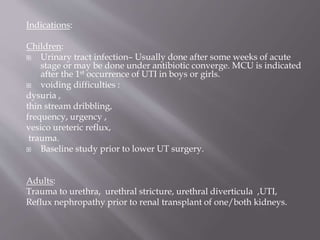

The voiding cystourethrogram is an x-ray exam used to evaluate the lower urinary tract. It involves inserting a catheter into the bladder and filling it with contrast dye before taking x-rays during urination. It can detect conditions like vesicoureteral reflux, bladder abnormalities, and issues with the bladder outlet. The document provides detailed information on how the exam is performed, what it can evaluate, common findings, and examples of various normal and abnormal results.