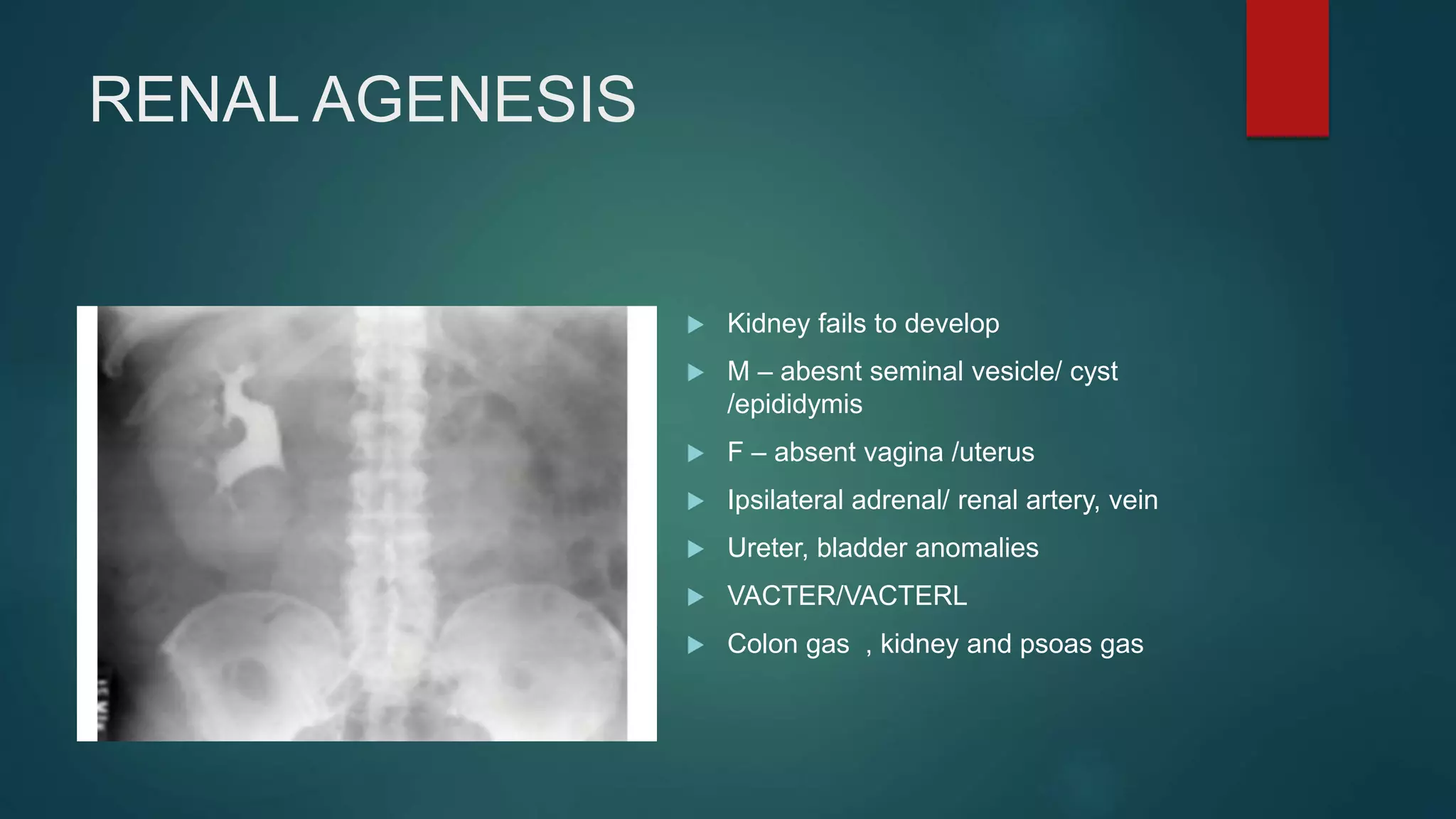
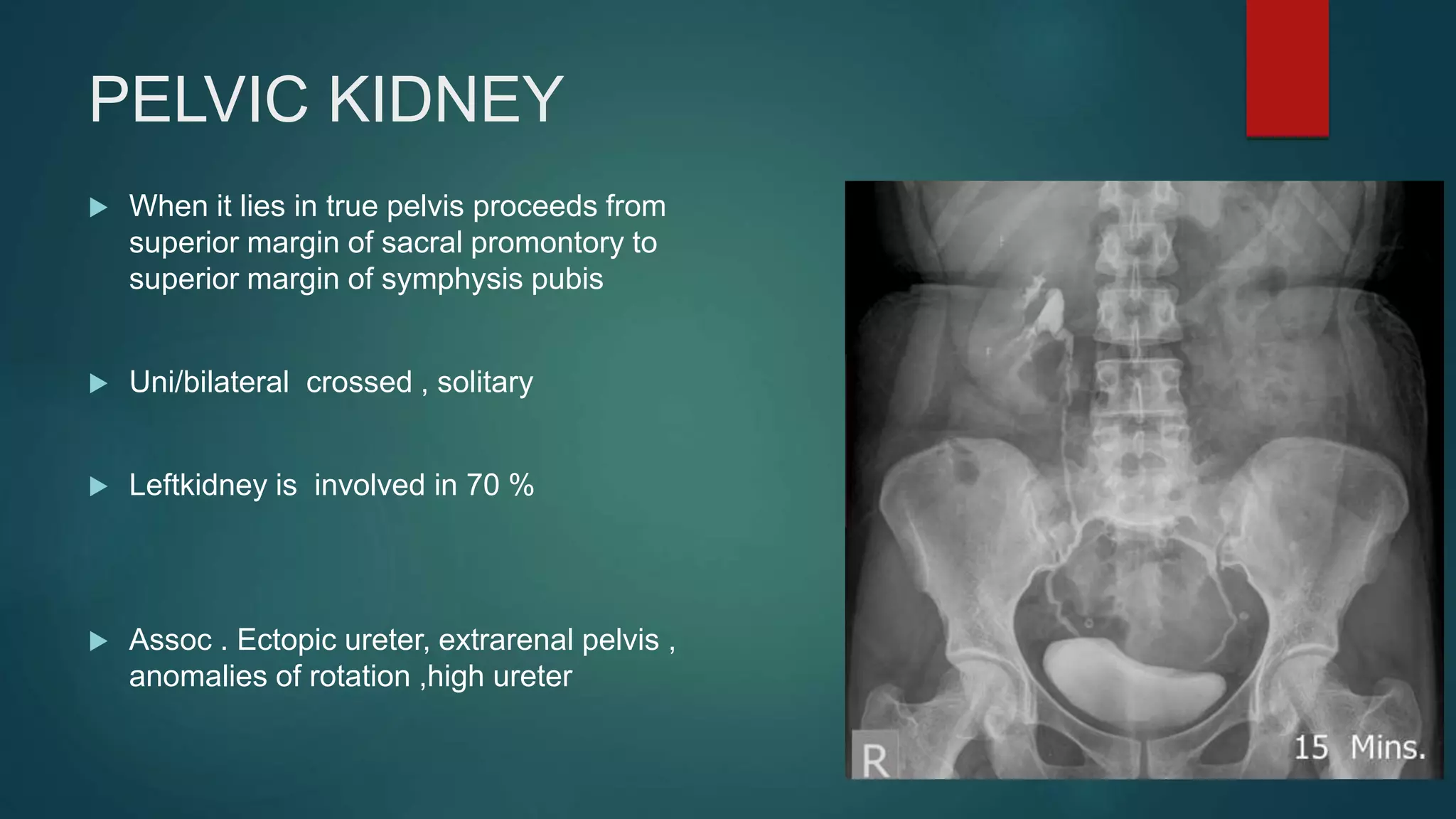
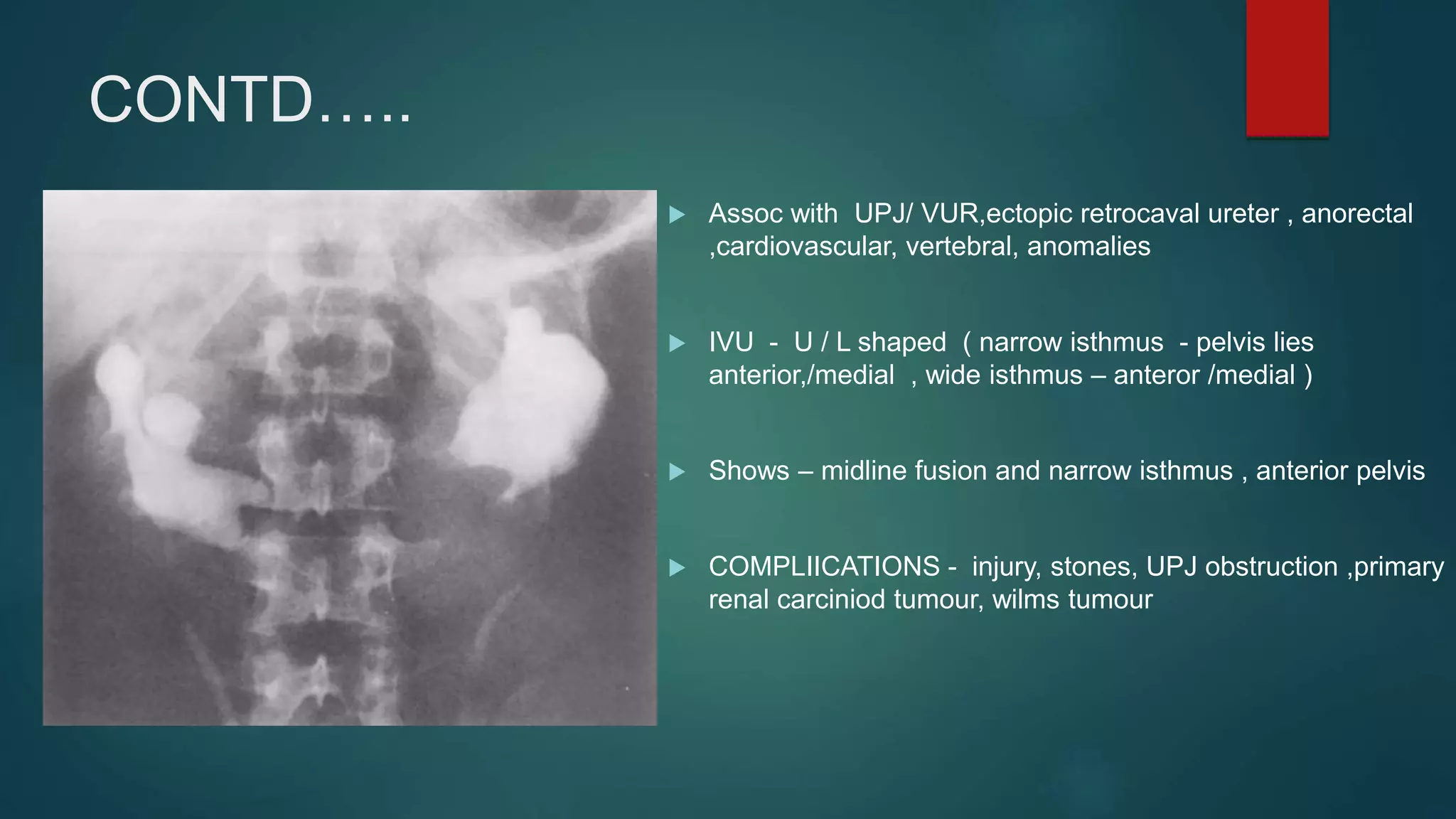
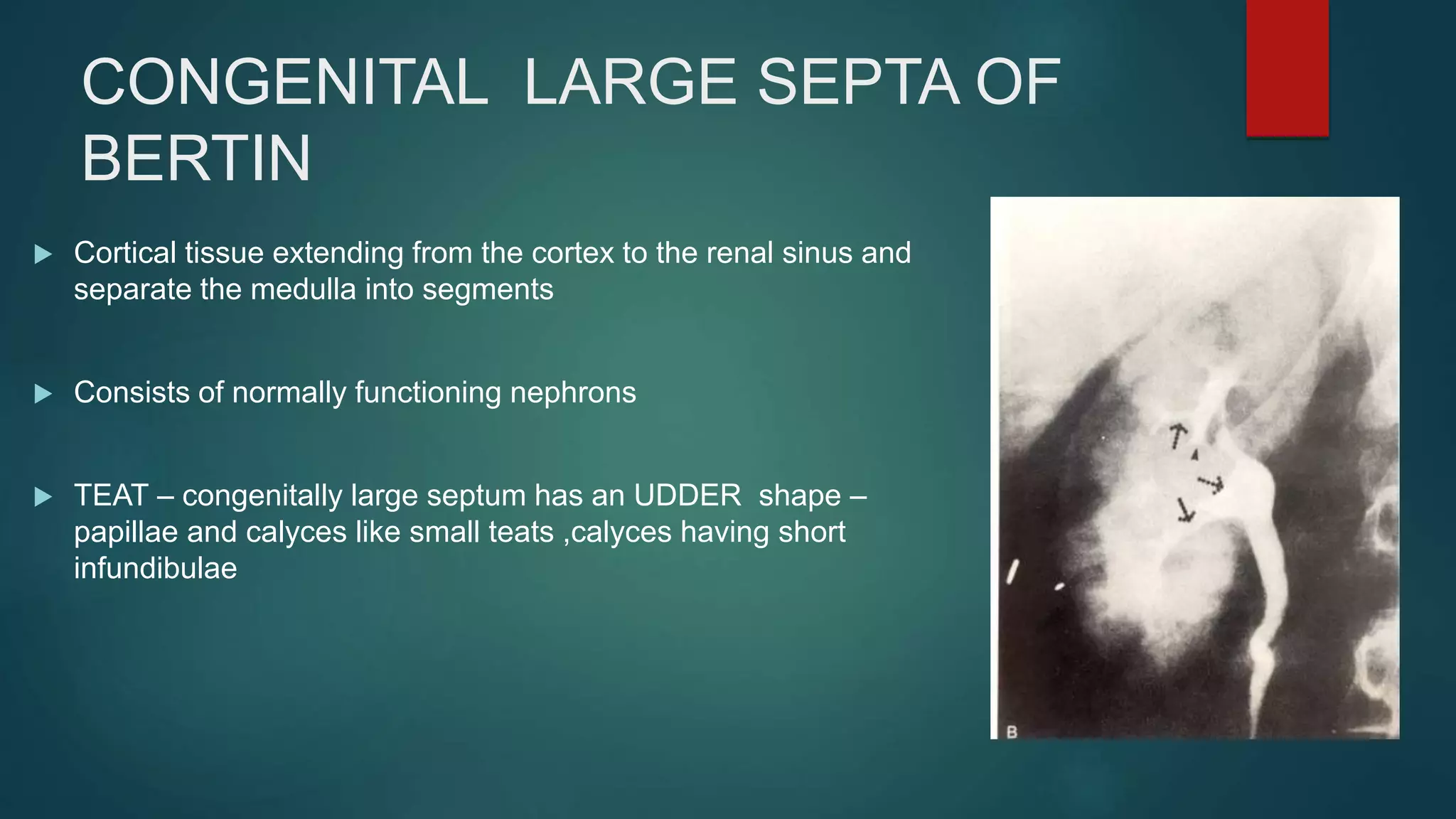
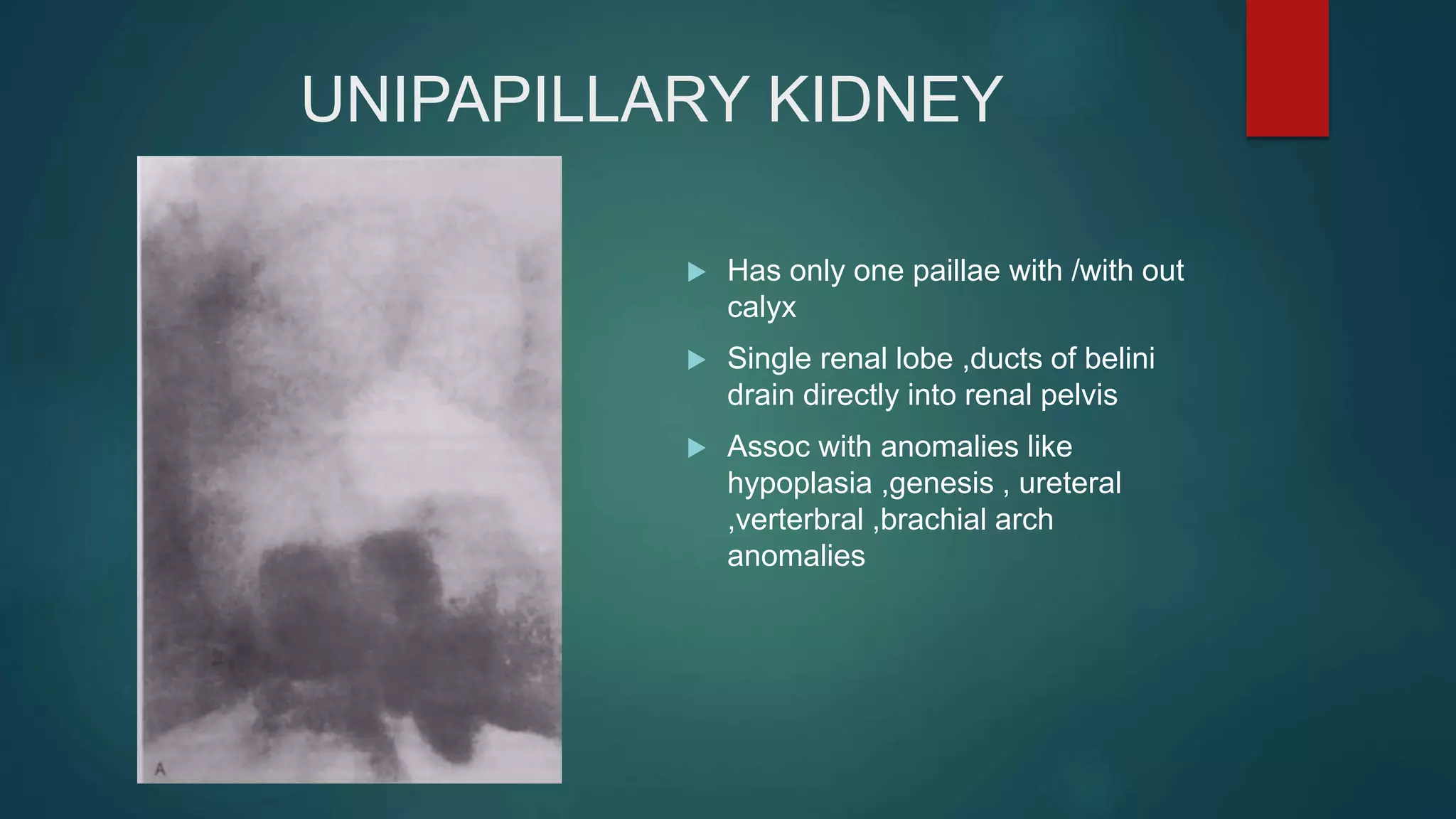
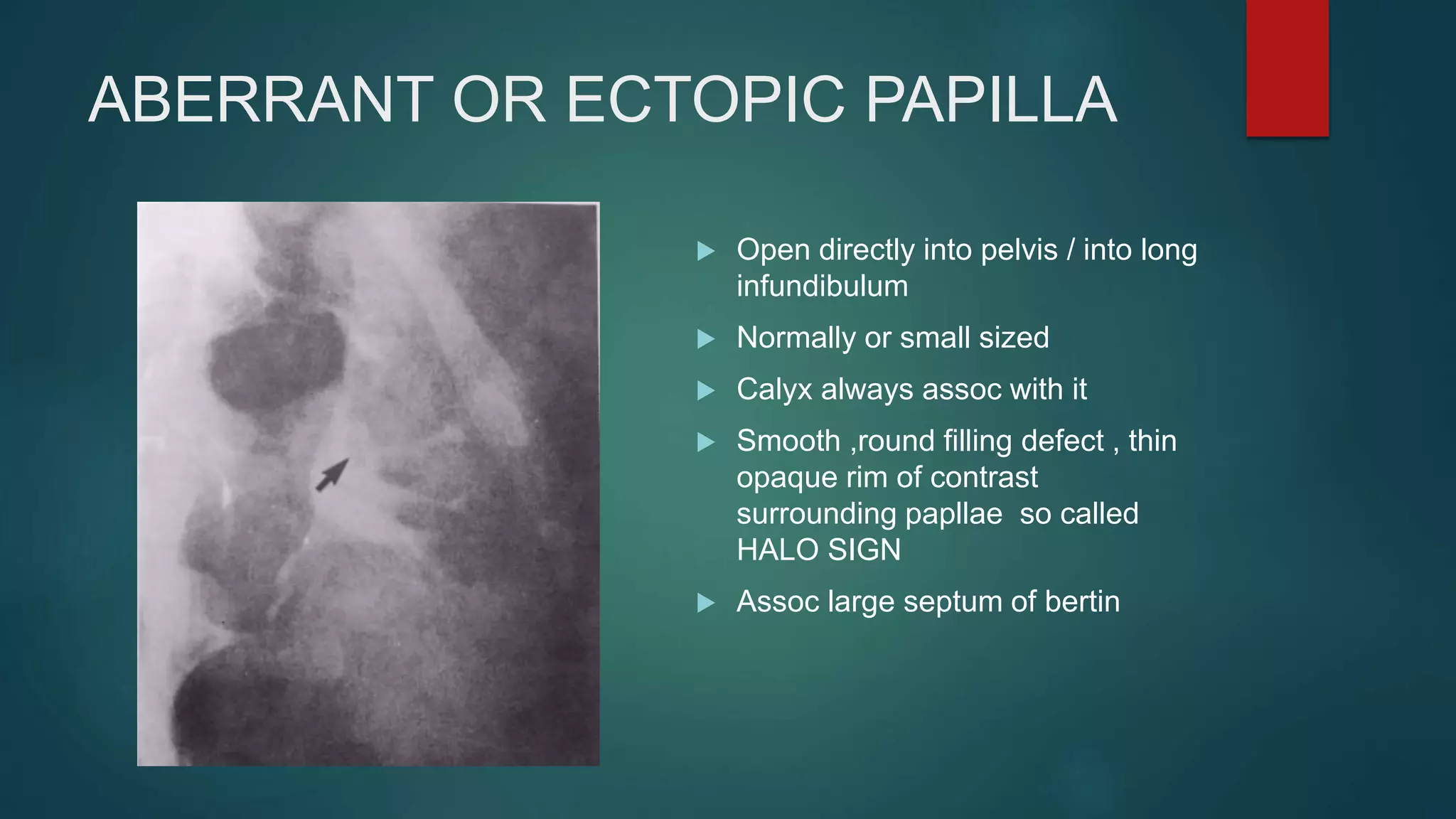
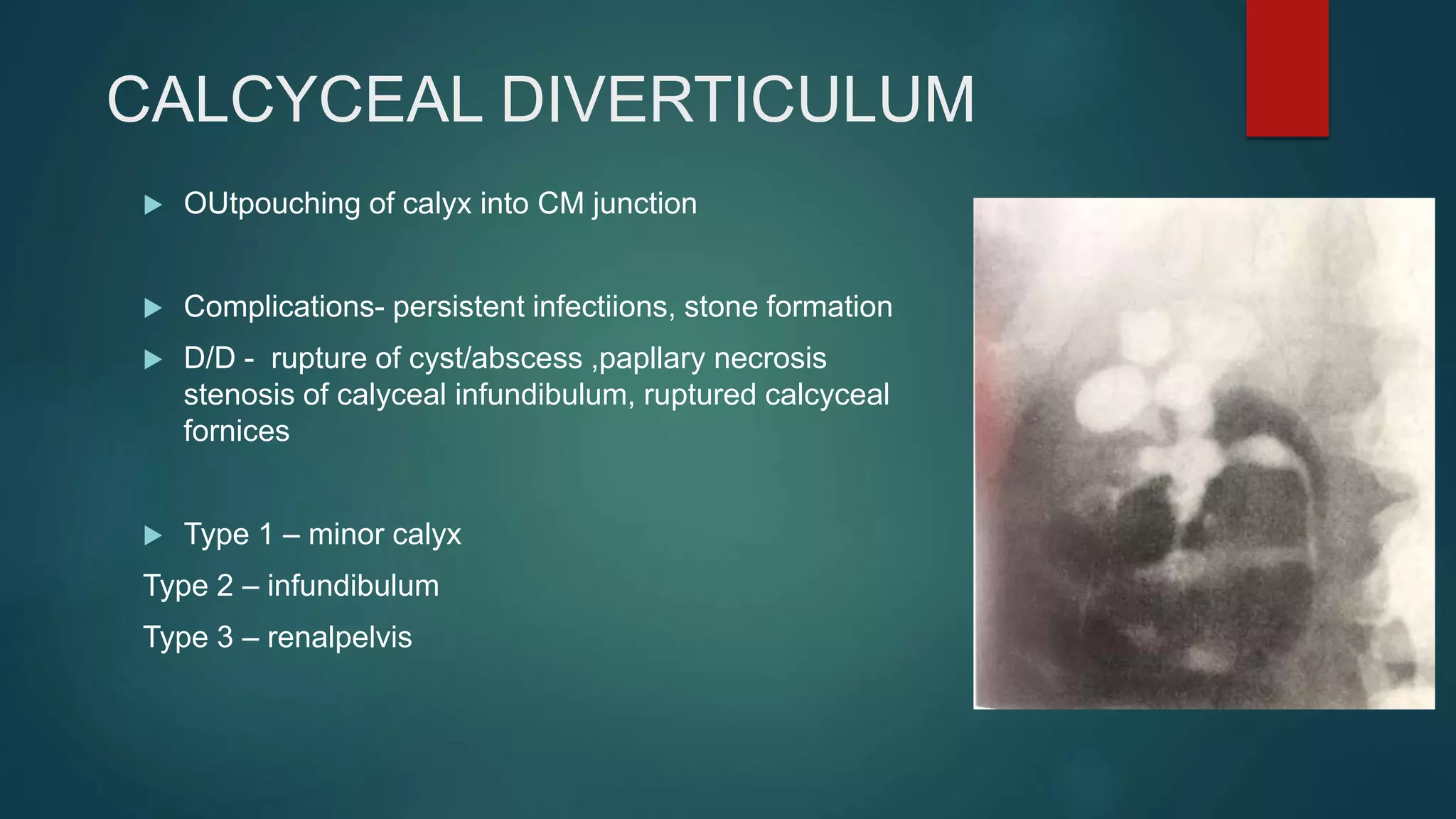
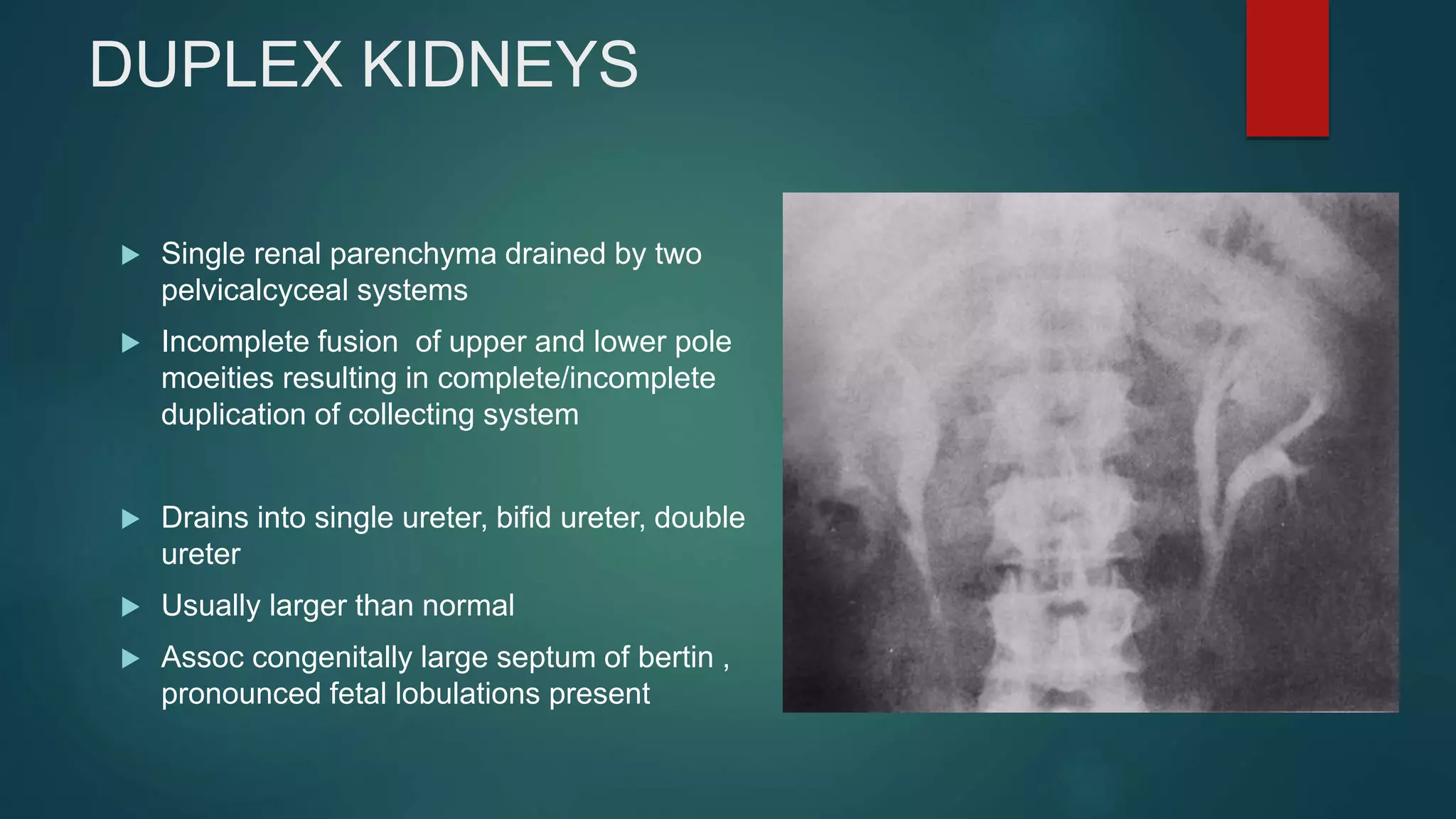
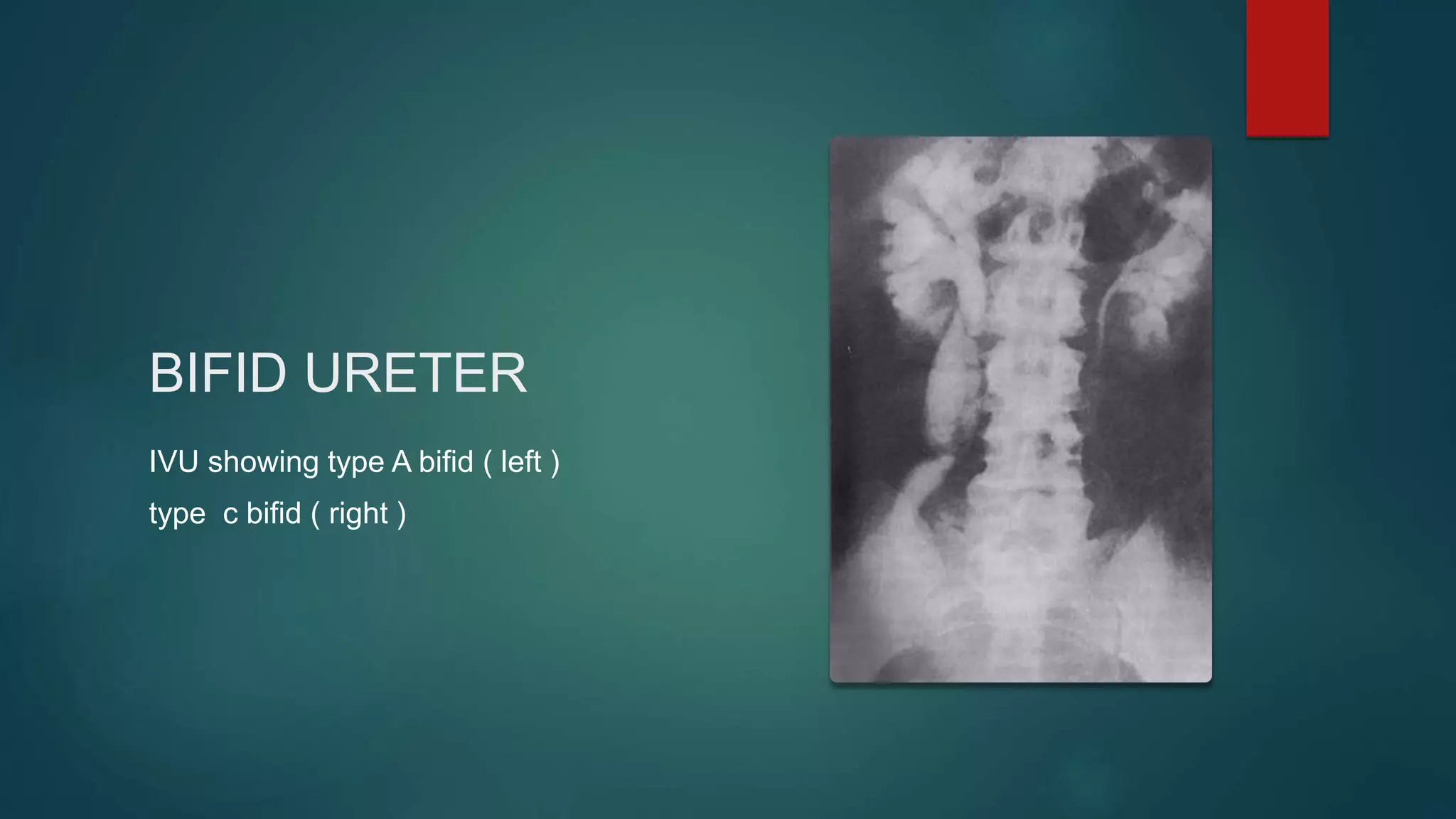
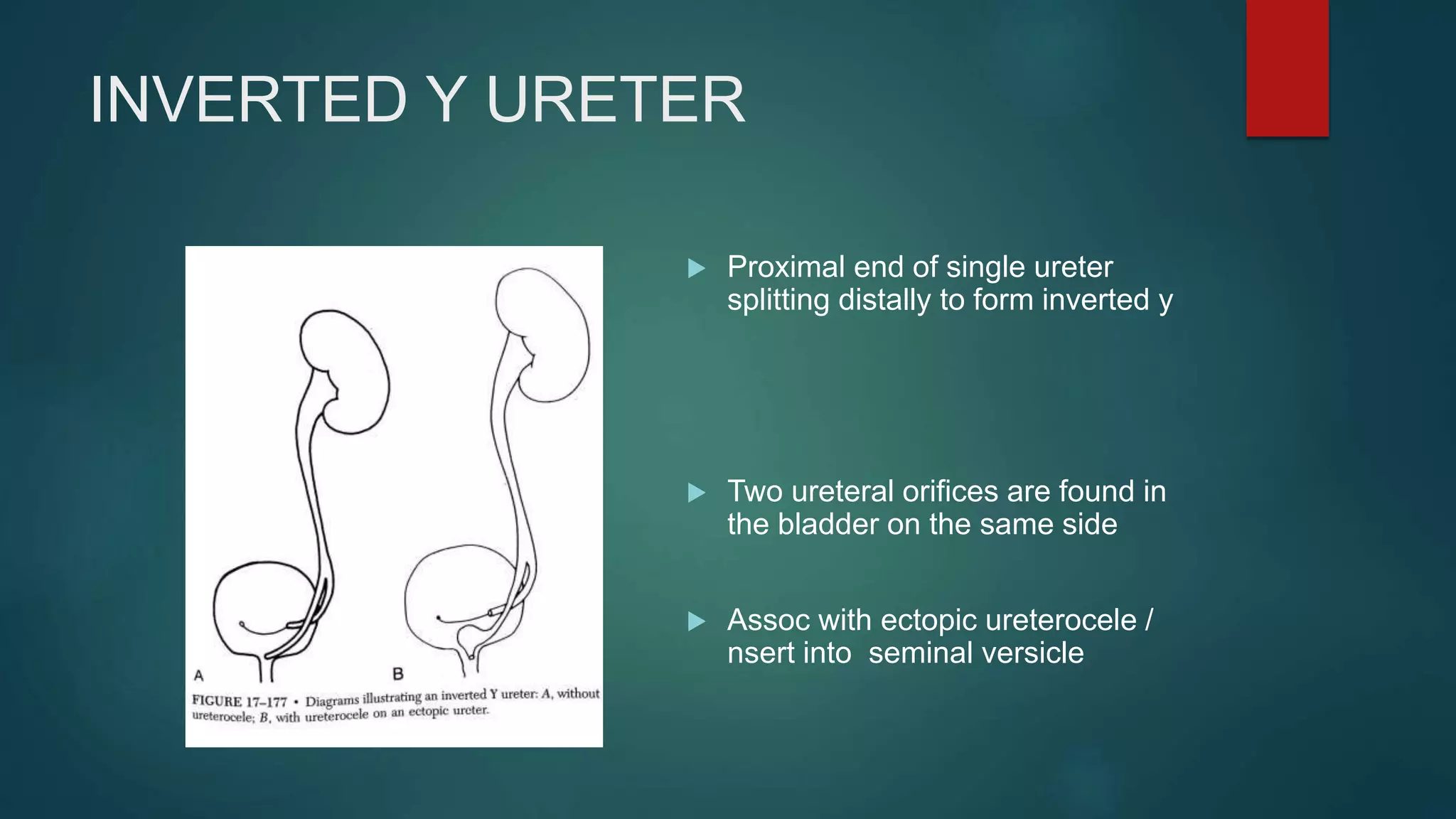
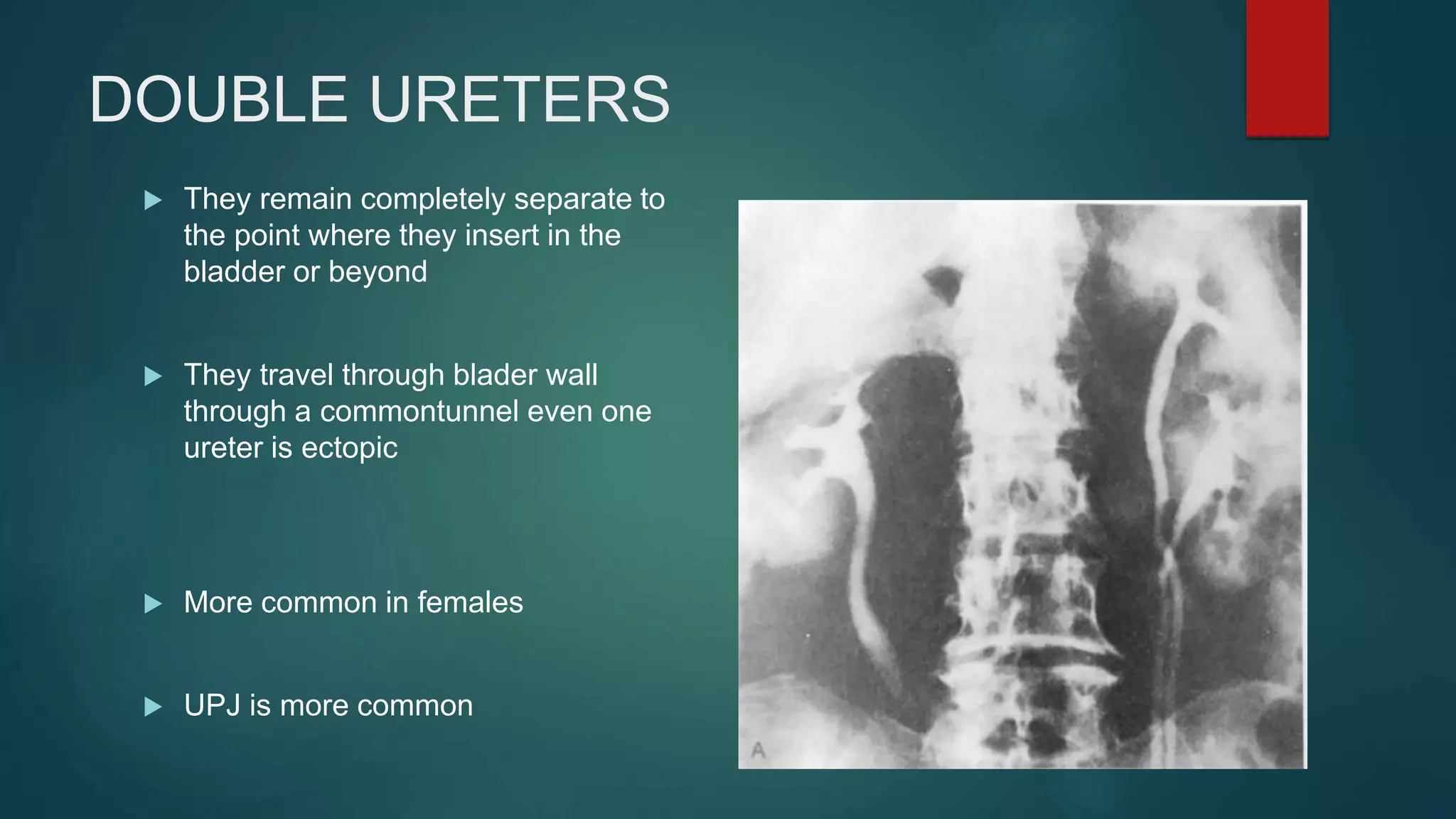
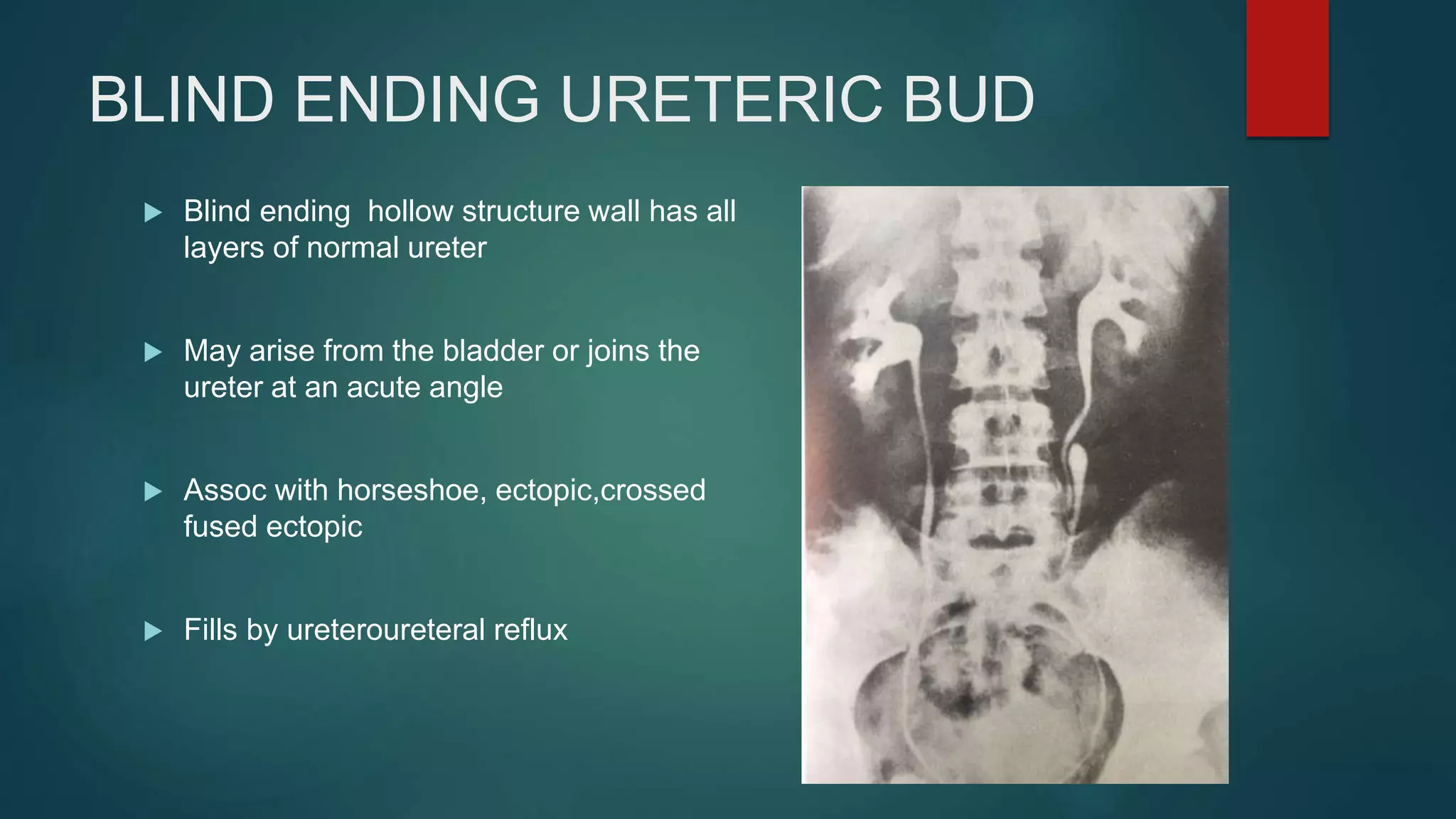
This document discusses various congenital kidney and urinary tract anomalies that can be seen on intravenous urograms (IVU). It describes abnormalities such as supernumerary kidneys, renal agenesis, renal hypoplasia, renal dysplasia, anomalies in kidney position including ectopia, horseshoe kidney, and anomalies in the renal pelvis and ureters including duplex kidneys and ureteroceles. Complications and distinguishing features of each anomaly are provided.