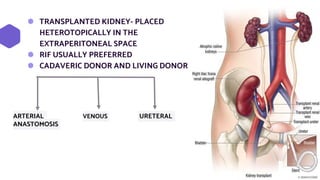
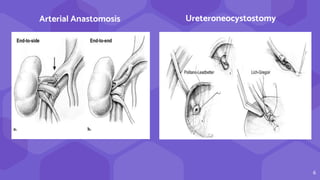
The document discusses imaging in renal transplantation, emphasizing the importance of pre- and post-operative imaging for diagnosing complications. It outlines various transplant techniques, analyzes risks for complications such as hematomas, lymphoceles, and vascular issues, and details diagnostic methods for monitoring graft function. Advanced imaging techniques like MRI and contrast-enhanced ultrasound are highlighted as essential adjuncts to routine surveillance using duplex ultrasound.