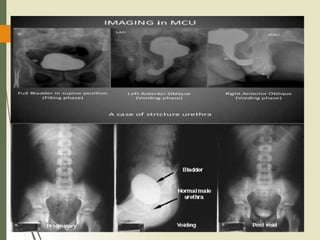
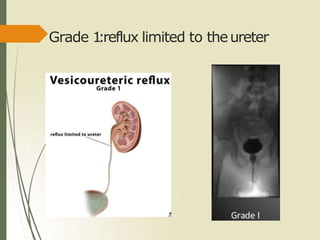
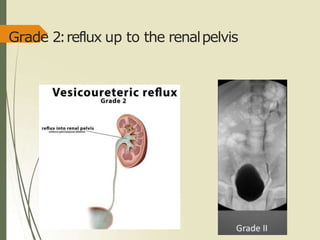
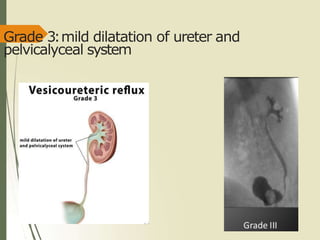
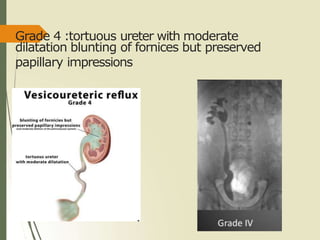
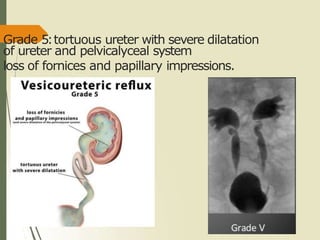
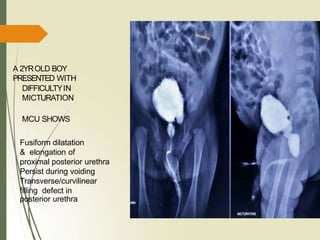
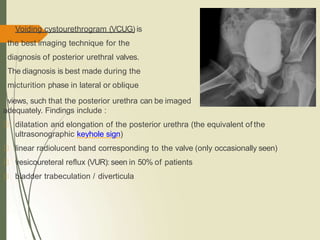
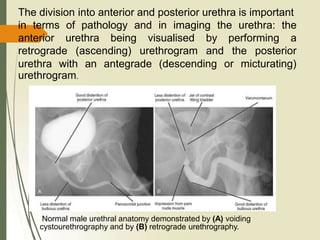
A MCU was performed on a 2-year-old child with a history of recurrent UTIs. The study identified vesicoureteric reflux (VUR), where urine flows back from the bladder into the ureters and kidneys. VUR was graded as [grade], indicating [description of grade]. In another case, a MCU was performed on a 2-year-old boy with difficulty urinating. This showed a fusiform dilatation and elongation of the proximal posterior urethra persisting during voiding, as well as a transverse filling defect, indicating the presence of posterior urethral valves. Posterior urethral valves are congenital folds of tissue in the posterior


![Formula for bladder capacity
For children>2 years
Bladder capacity in ml= ( Age[years] + 2 )X
30
For children< 2 years
Bladder capacity in ml= weight[kg] X 7
Adult: around 500 ml](https://image.slidesharecdn.com/vcuppt-201219102430/85/Vcu-ppt-19-320.jpg)