Downloaded 627 times



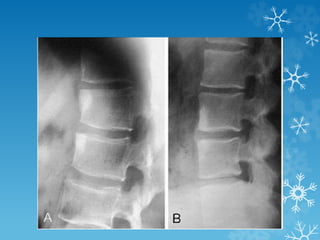
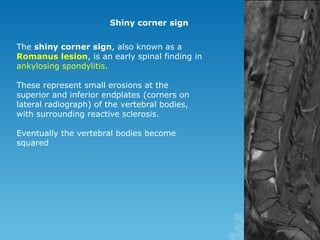


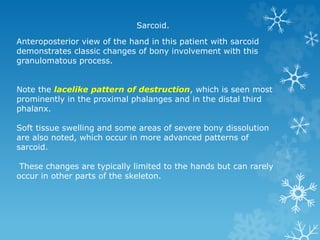


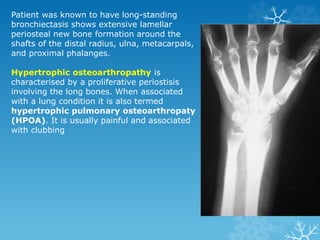










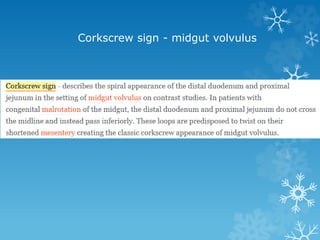















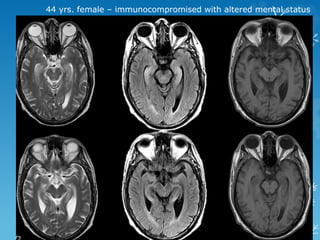

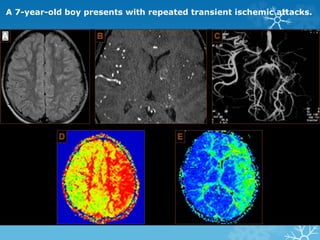
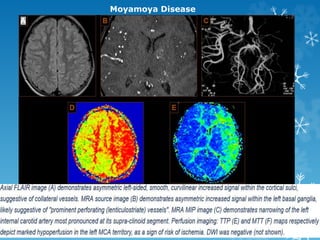


This document contains descriptions of various medical imaging findings and cases. Some key points summarized: - Spot 1 describes shiny corner signs seen in ankylosing spondylitis on x-ray. Spot 2 shows bone changes in the hands seen in sarcoidosis. Spot 3 shows periosteal bone formation associated with hypertrophic pulmonary osteoarthropathy. - Several spots name common imaging signs and their associated diagnoses, such as the corkscrew sign seen in midgut volvulus in Spot 10. - Case 2 describes a immunocompromised patient with altered mental status, showing findings of toxoplasmosis. Case 6 shows imaging and diagnosis of Moyamoya disease in a




































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)
![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)

















