Downloaded 185 times

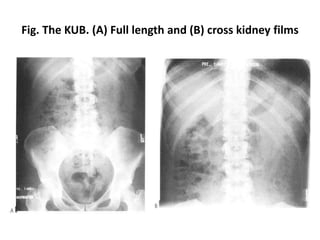


This document discusses imaging of the urinary tract, including KUB (kidneys, ureters, bladder) radiography and intravenous urography (IVU). It provides details on: - The standard KUB technique using two abdominal x-ray images to outline the kidneys, ureters and bladder. - The classic IVU procedure involving a series of x-ray images before and after intravenous injection of iodine contrast to visualize the functioning of the kidneys and urinary tract. - Modifications of IVU for specific situations like urinary obstruction or pregnancy to minimize radiation exposure.























































































