Downloaded 67 times
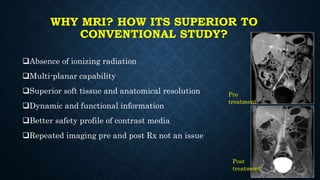
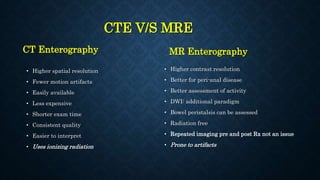
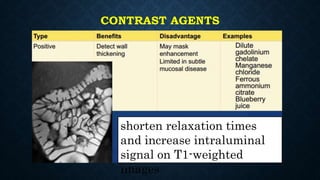
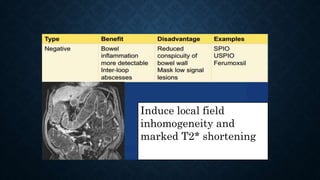
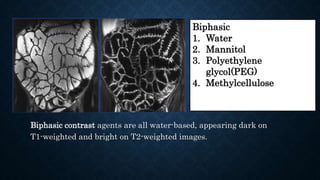
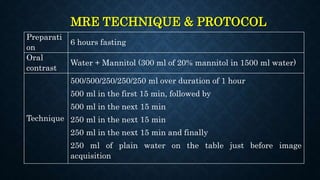
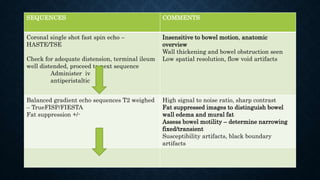
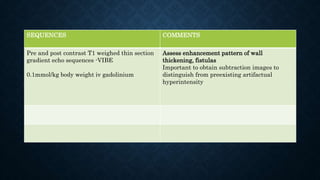

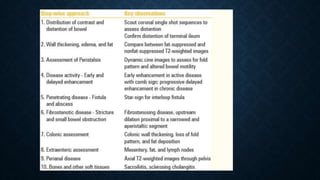
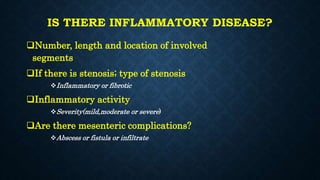
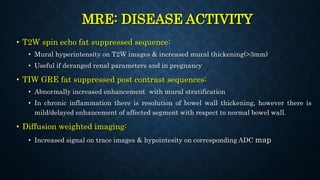

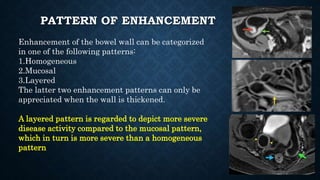
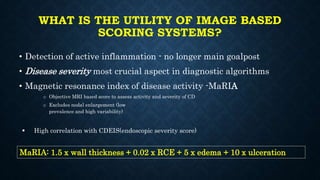

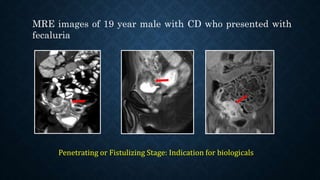




MR enterography/enteroclysis is a non-invasive technique used to diagnose small bowel disorders. Enterography involves oral contrast, while enteroclysis uses a nasoenteric tube. MR enterography offers multiplanar imaging and functional data without radiation. It is superior to CT for assessing peri-anal disease and bowel peristalsis. Indications include Crohn's disease, tuberculosis, and neoplasms. Contrast agents improve luminal visualization. Techniques involve prone positioning, antiperistaltic drugs, and pre- and post-contrast sequences. Findings are used to characterize inflammation, activity, complications and differentiate conditions like tuberculosis from Crohn's disease. Scoring systems like MaRIA objectively assess
























































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)
![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)









