Downloaded 48 times
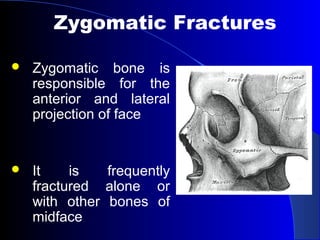



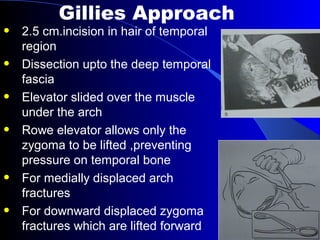

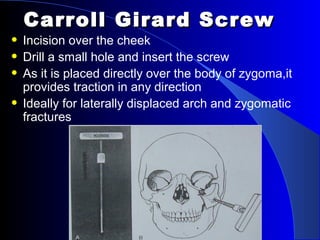
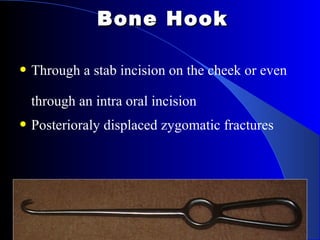
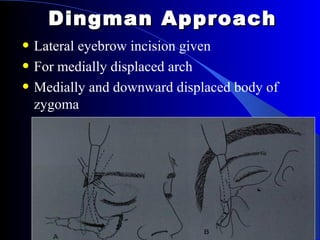




This document discusses reduction techniques for zygomatic bone fractures. It begins by describing the anatomy of the zygomatic bone and common types of zygomatic fractures. It then outlines various surgical approaches that can be used for open reduction of zygomatic fractures, including the temporal fossa, intraoral, percutaneous, malar hook, Carroll Girard screw, and lateral eyebrow approaches. Indications for surgery include depressed malar eminence, enophthalmos, infraorbital paresthesia, and inability to open the mouth. The conclusion recommends that technique choice depends on the location and degree of displacement of the fracture.











































































































