Downloaded 2,108 times
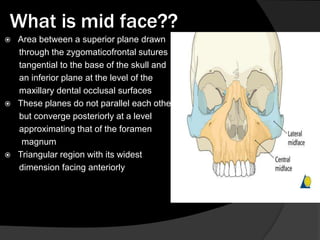
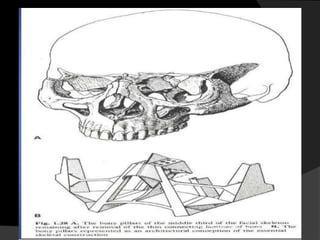
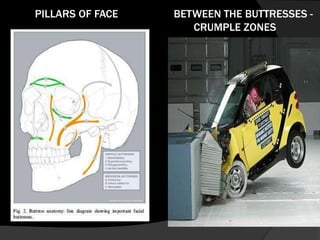
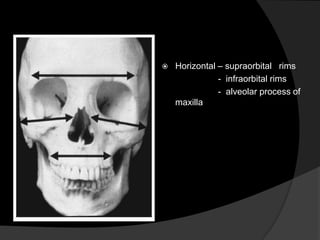
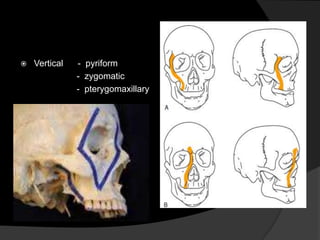
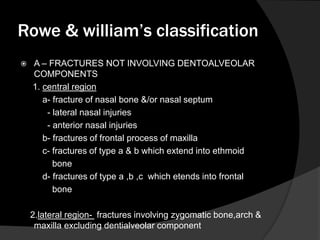
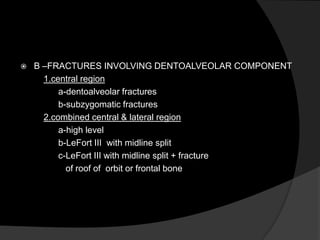
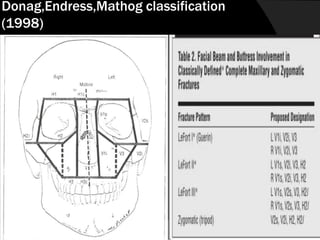
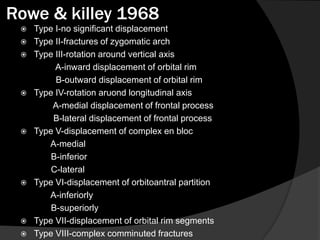
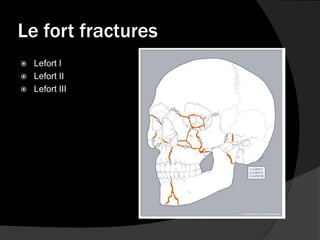
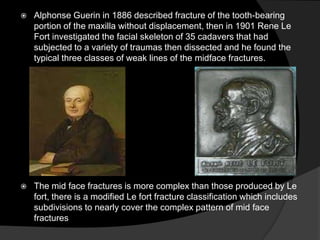
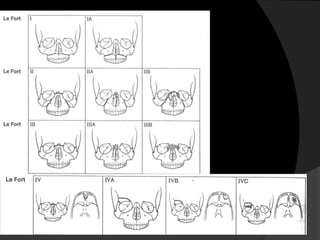
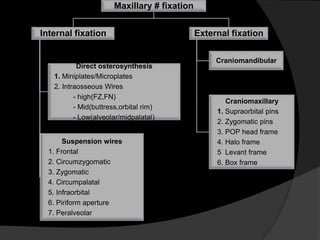
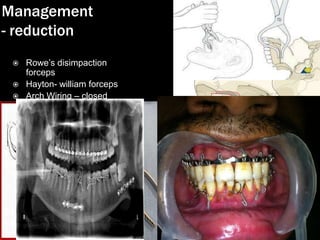


The document provides an overview of midface anatomy, its bony structures, and emphasizes the complexity of midface fractures and their classifications, including Le Fort and modified Le Fort fractures. It outlines various diagnostic imaging techniques and treatment principles, including reconstruction strategies and internal fixation methods for stabilizing fractures. Additionally, it discusses the effects of fractures on facial aesthetics and function alongside the surgical approaches for management.













































































