Downloaded 37 times













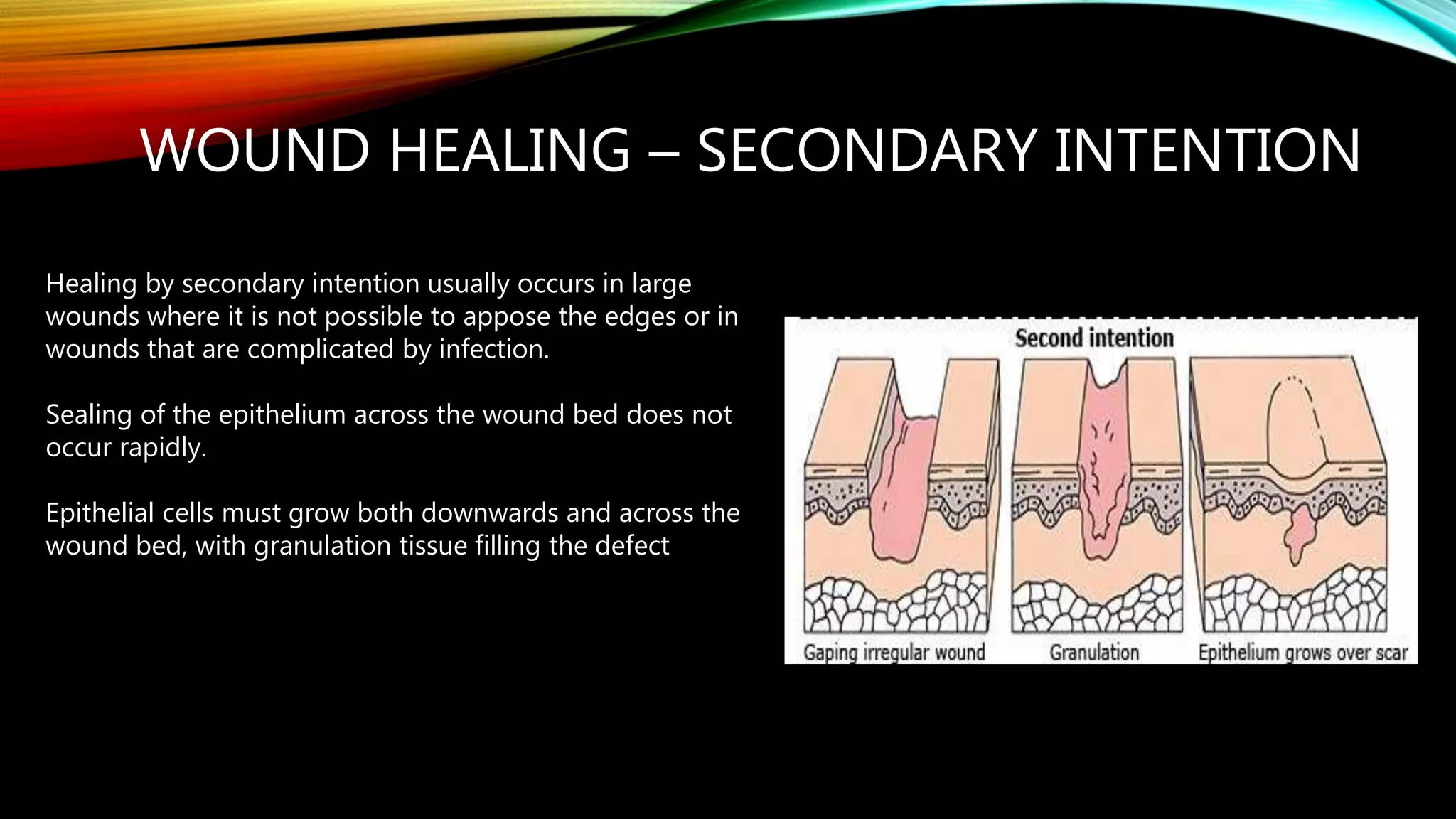




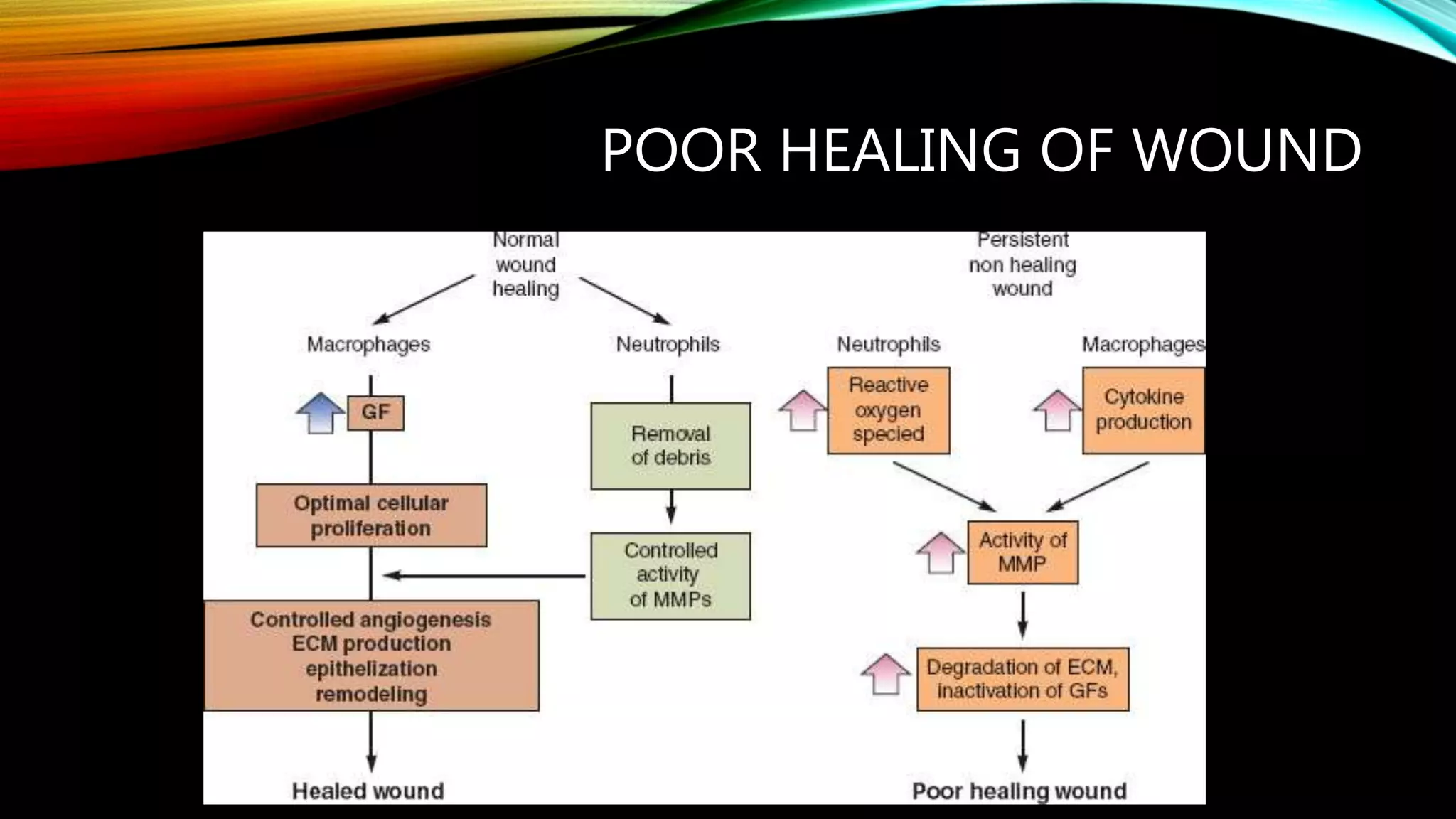






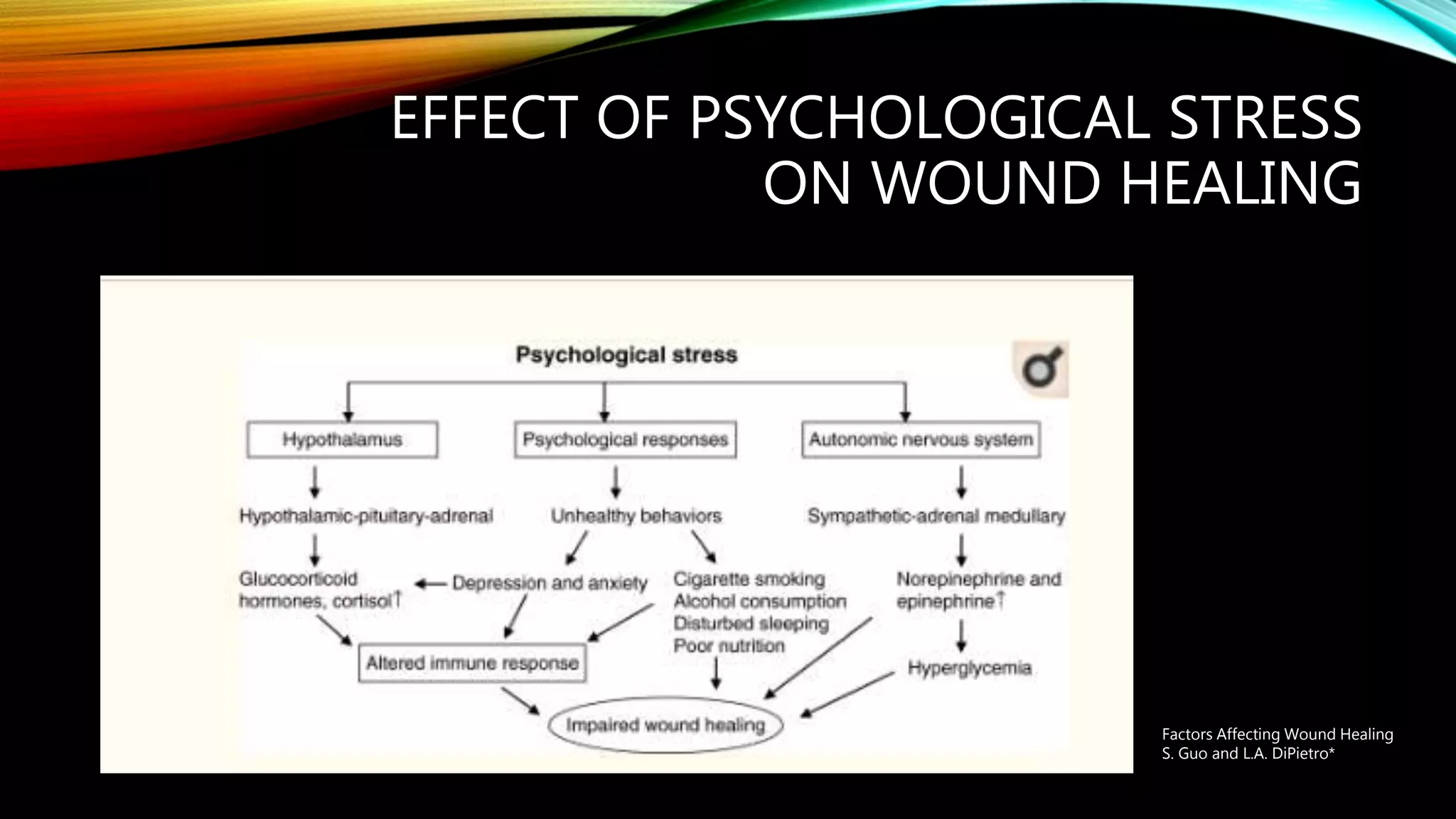

















This document discusses wound healing and provides information on various topics related to wound management. It begins with introducing wounds and the stages of wound healing. It then covers skin anatomy, functions of skin, and the different types of wounds. The document discusses wound healing through primary and secondary intention. It also addresses factors that can interfere with or impede wound healing such as infection, diabetes, obesity, and psychological stress. The document provides guidance on assessing wounds and managing acute wounds. It concludes by covering complications of wound healing.














































![4_5933593097194704354[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/459335930971947043541-230123122719-1e0eaf18-thumbnail.jpg?width=640&height=640&fit=bounds)








































