Downloaded 41 times







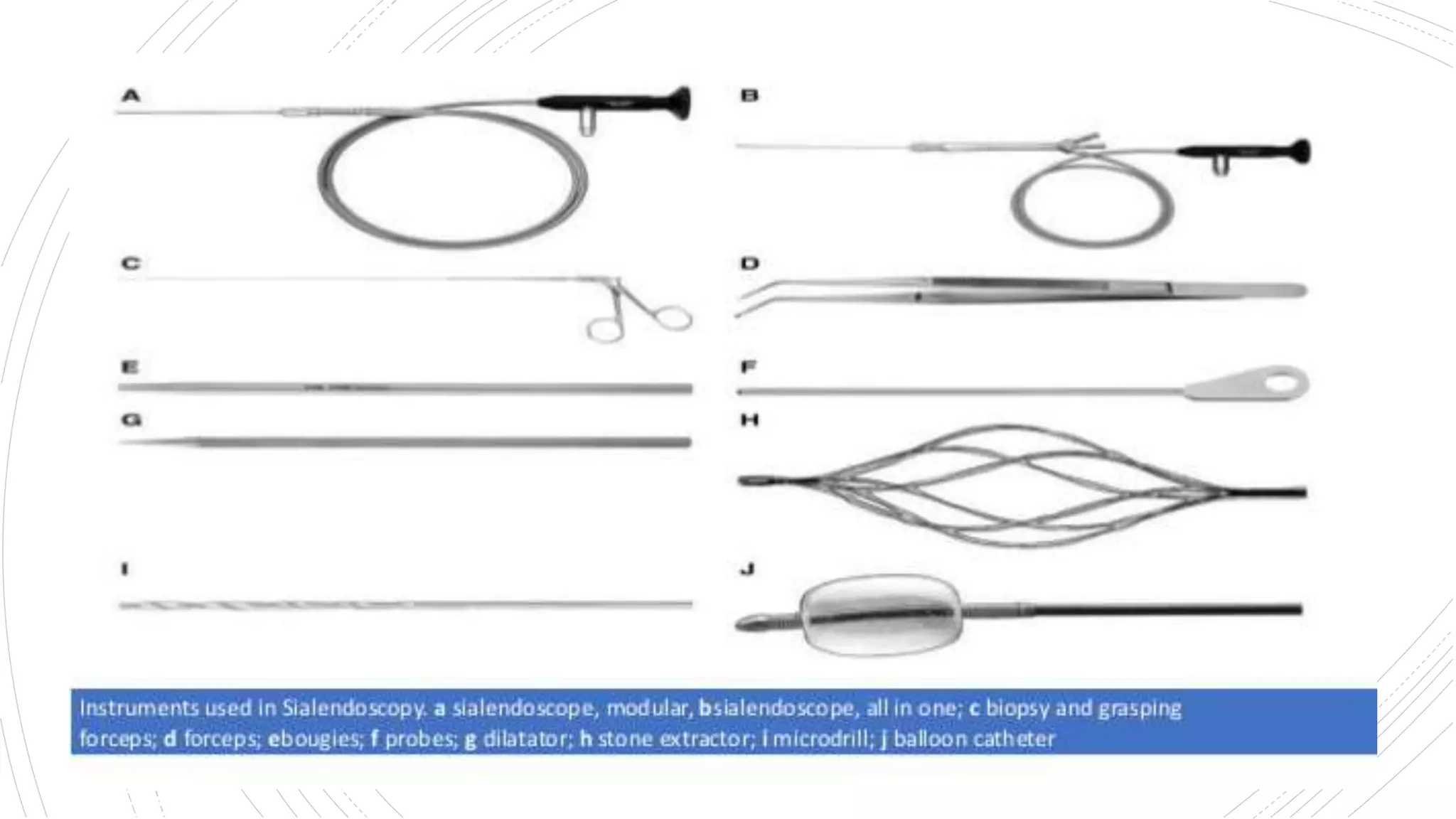



















Sialendoscopy is a minimally invasive endoscopic technique used to both diagnose and treat salivary gland disorders. Some key developments in sialendoscopy include Katz introducing a flexible endoscope in 1991 to diagnose and treat salivary gland stones. Sialendoscopy uses thin endoscopes and mini instruments to visualize and treat obstructive pathologies like sialoliths, strictures, ductal polyps and mucous plugs in the major salivary glands. It allows for direct visualization of the ductal system and less invasive interventional procedures compared to open surgery. Complications can include local pain, lingual nerve changes, infection and ductal strictures.























































































