Downloaded 162 times

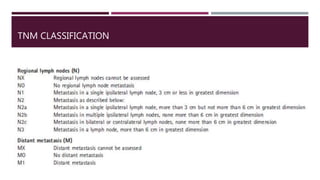
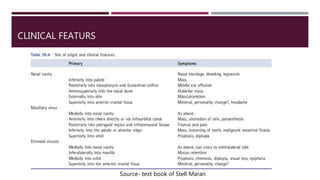
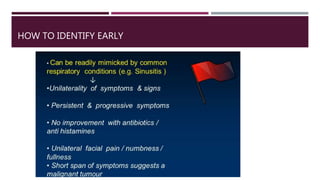
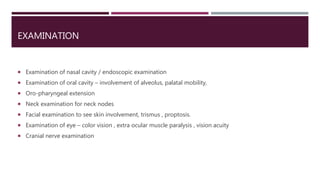
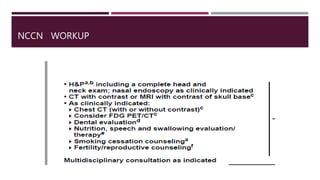
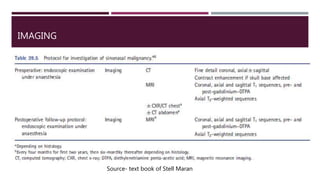
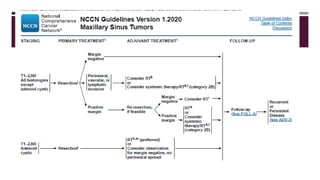
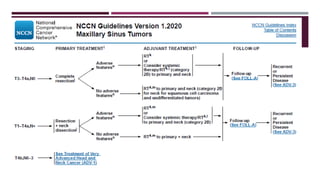
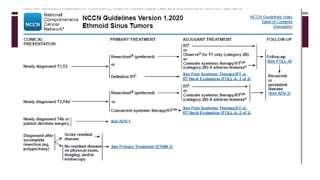
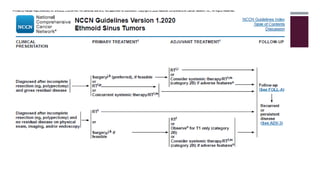


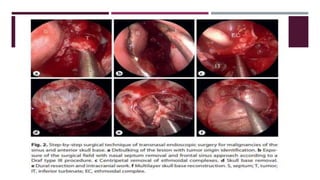
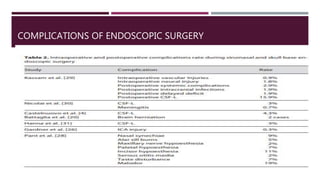
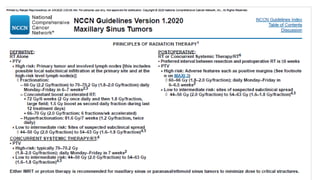
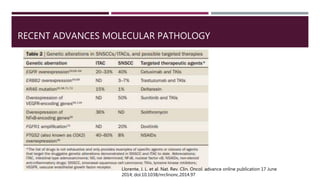

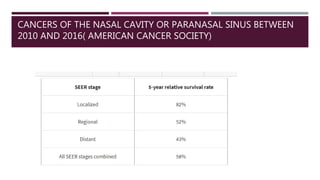
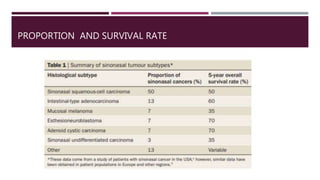


This document provides an overview of sinonasal malignancy including: - The complex surgical anatomy of the sinonasal region and proximity to vital structures. - The histopathological classification and TNM staging of sinonasal cancers. - Presentation, diagnosis, and multidisciplinary management approaches including endoscopic surgery, radiotherapy, and imaging. - Specific details are provided on surgical procedures like craniofacial resection and midfacial degloving for advanced tumors.























































































