Downloaded 38 times










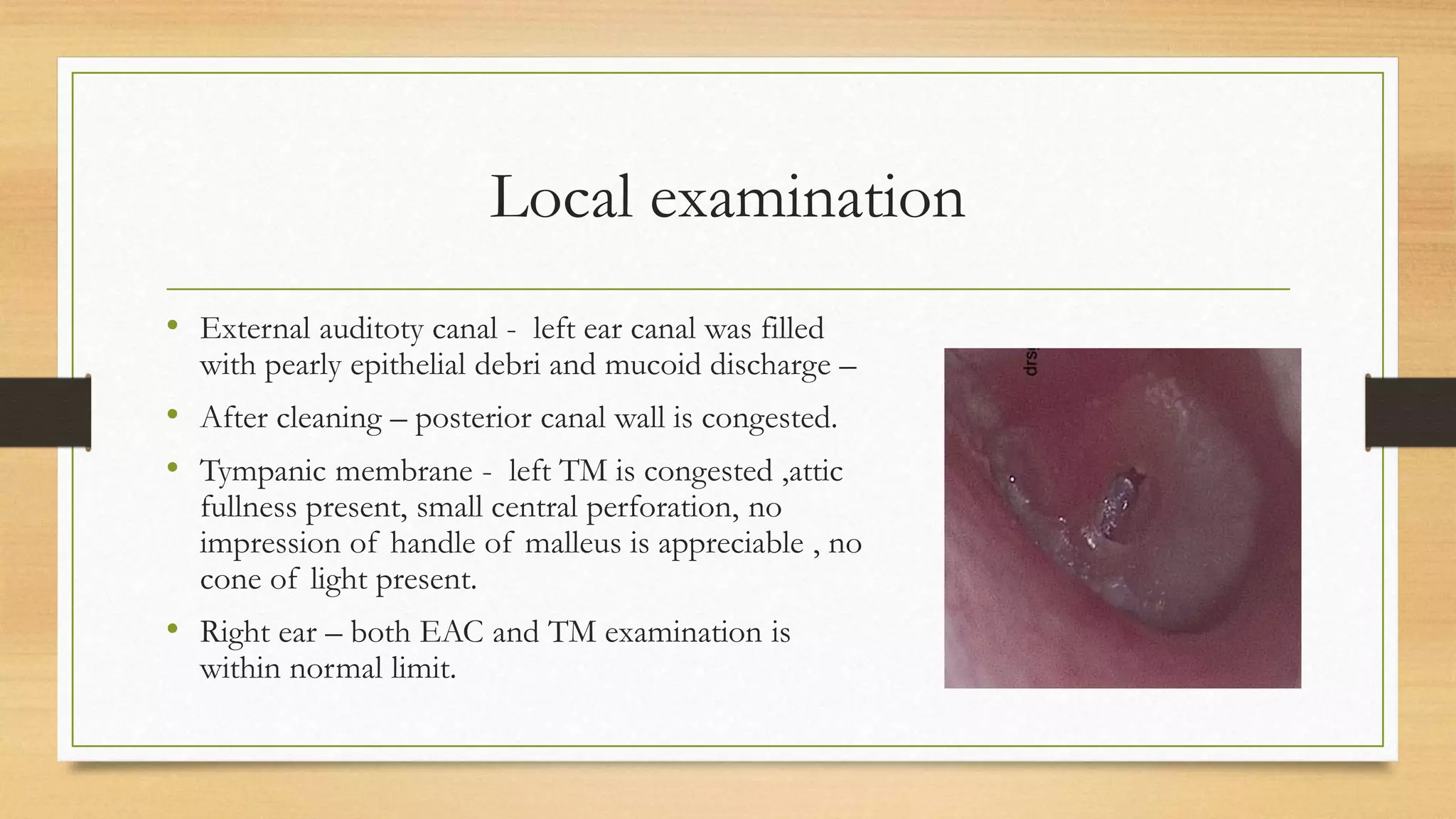











The document presents a case of a 7-year-old female patient with chronic otitis media, characterized by persistent discharge from the left ear and progressive hearing loss over two years. Despite multiple courses of antibiotics, the discharge remained unchanged, with notable findings during local examination including a central perforation and congested tympanic membrane. The proposed management plan includes canal wall down mastoidectomy with ossiculoplasty and grafting.























































































