Acute allergic conjunctivitis–
presentation
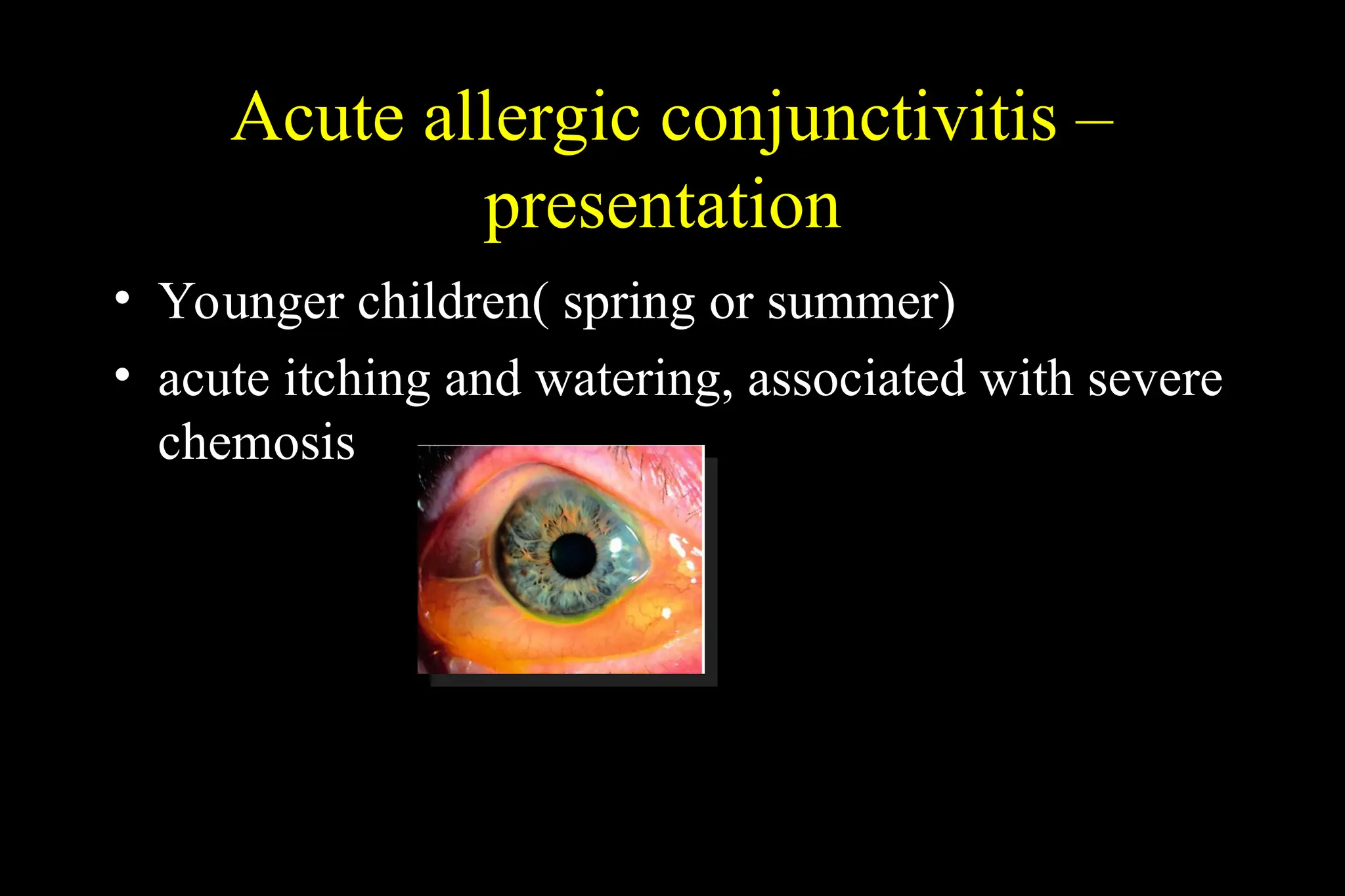
• Younger children( spring or summer)
• acute itching and watering, associated with severe
chemosis
4.
Acute allergic conjunctivitis–
treatment
• Usually not require
– Chemosis settle within hours
• Cool compress
• Single drop of adrenaline 1%
5.
Seasonal and perennialallergic
conjunctivitis
Seasonal”hay fever eye “
• Spring and summer
• Allergen: tree and grass
polen
• Specific allergen varies
with geographic location
• Common
Perennial
• Through the year, worst in
automm
• Allegen: house dust mite,
animal dander, fungal
allergen
• Less common
6.
Diagnosis
• Presentation: transientacute or subacute redness, watering and itching,
associated with sneezing or nasal discharge
• Signs:
– completely resolve within episode
– Conjunctival hyperemia
– Mild papillary reaction
– Chemosis and eyelid edema
• Investigation
– Not require
– Conjunctival scrapping -> eosinophilia
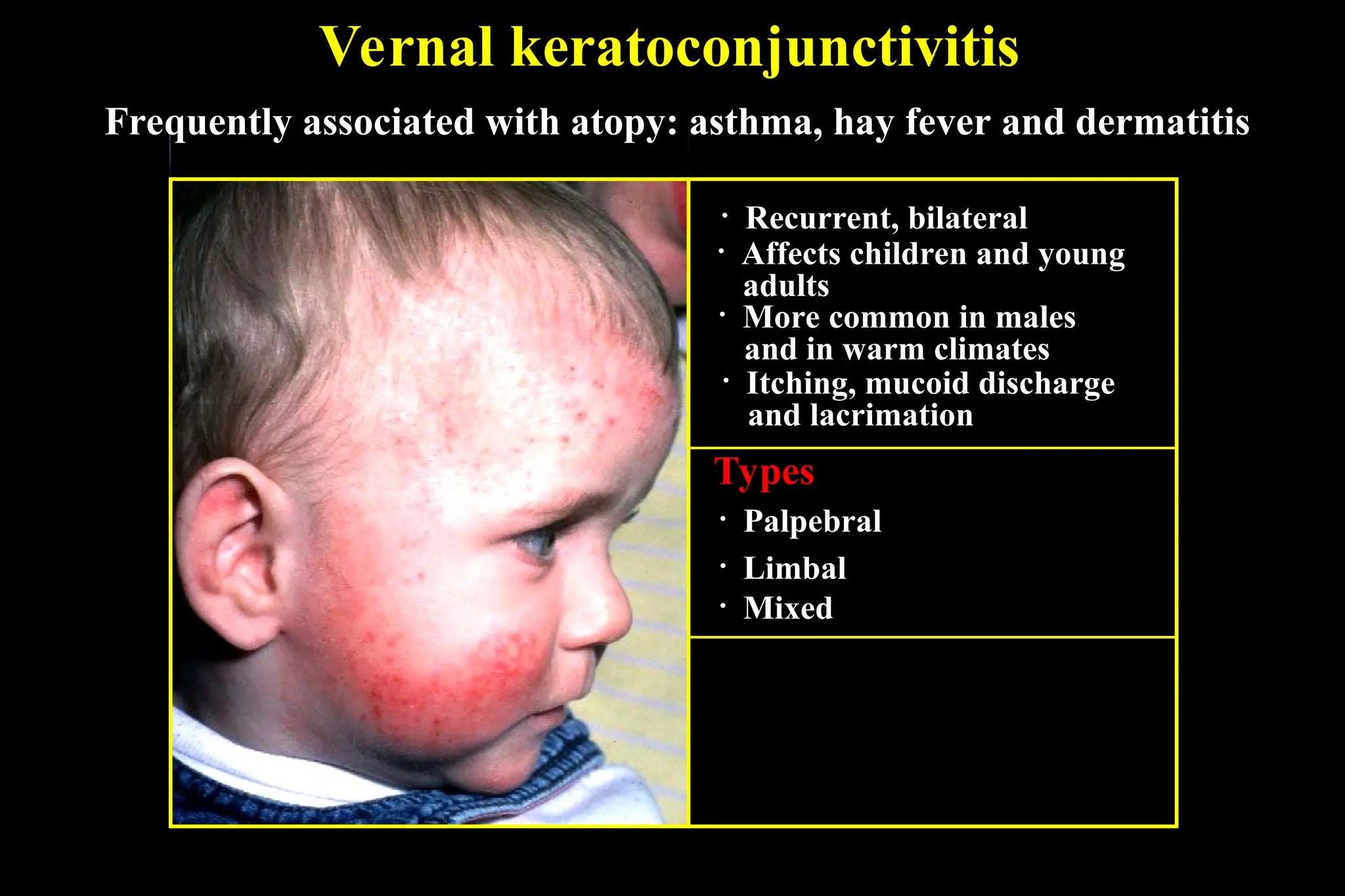
Vernal keratoconjunctivitis
• Affectschildren and young
adults
• More common in males
and in warm climates
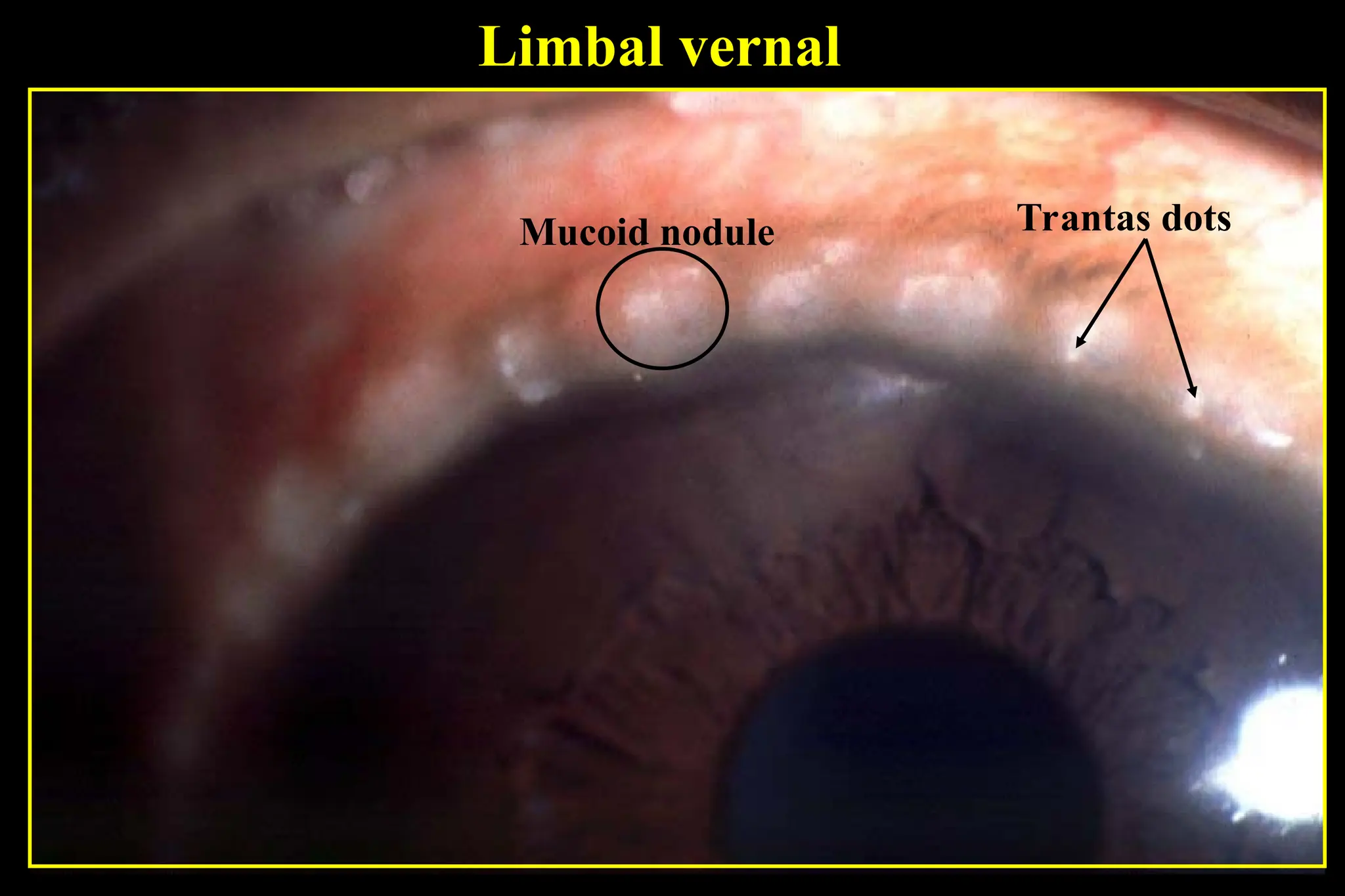
• Itching, mucoid discharge
and lacrimation
• Palpebral
Types
• Limbal
• Mixed
• Recurrent, bilateral
Frequently associated with atopy: asthma, hay fever and dermatitis
9.
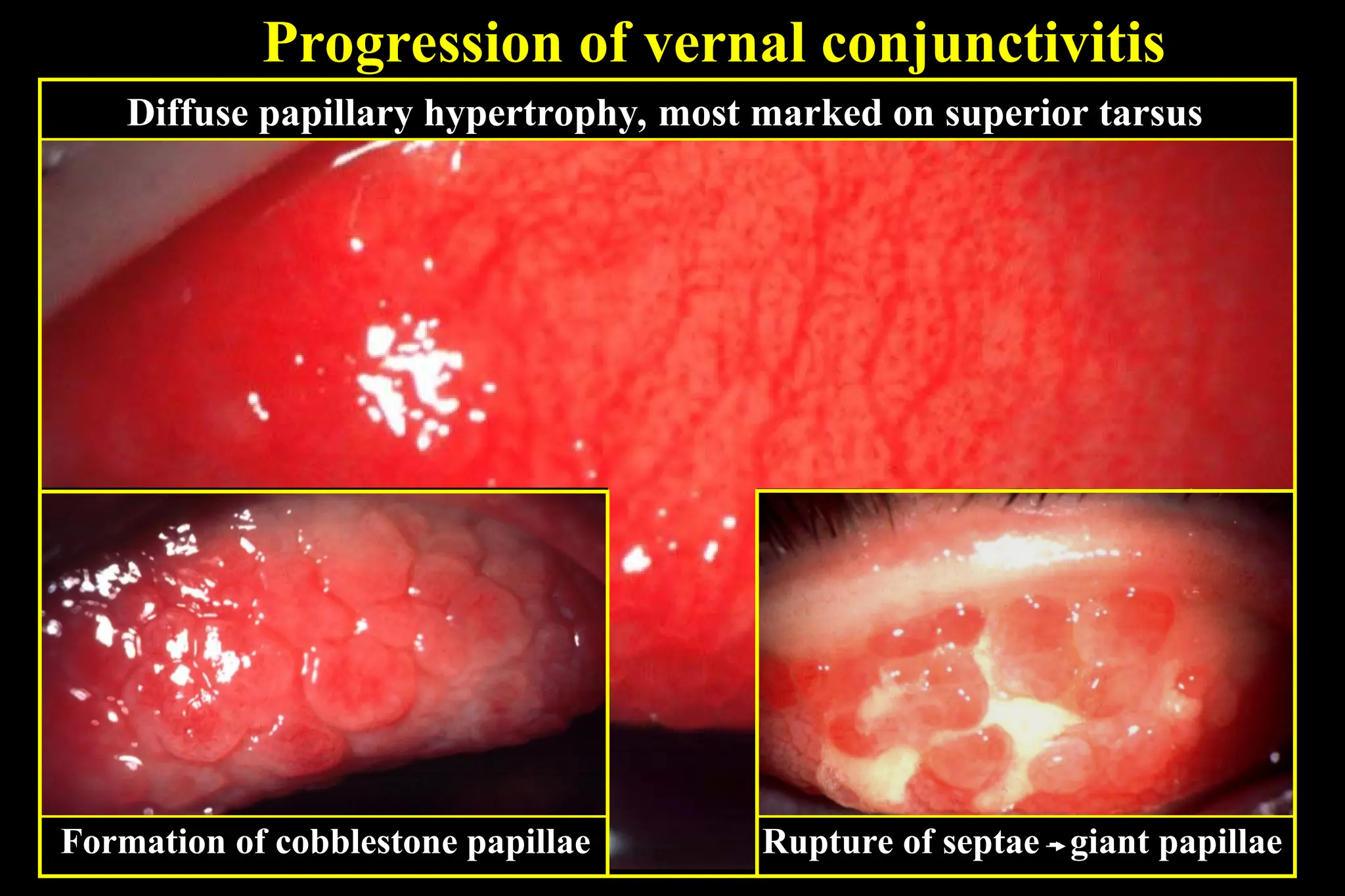
Progression of vernalconjunctivitis
Diffuse papillary hypertrophy, most marked on superior tarsus
Formation of cobblestone papillae Rupture of septae - giant papillae
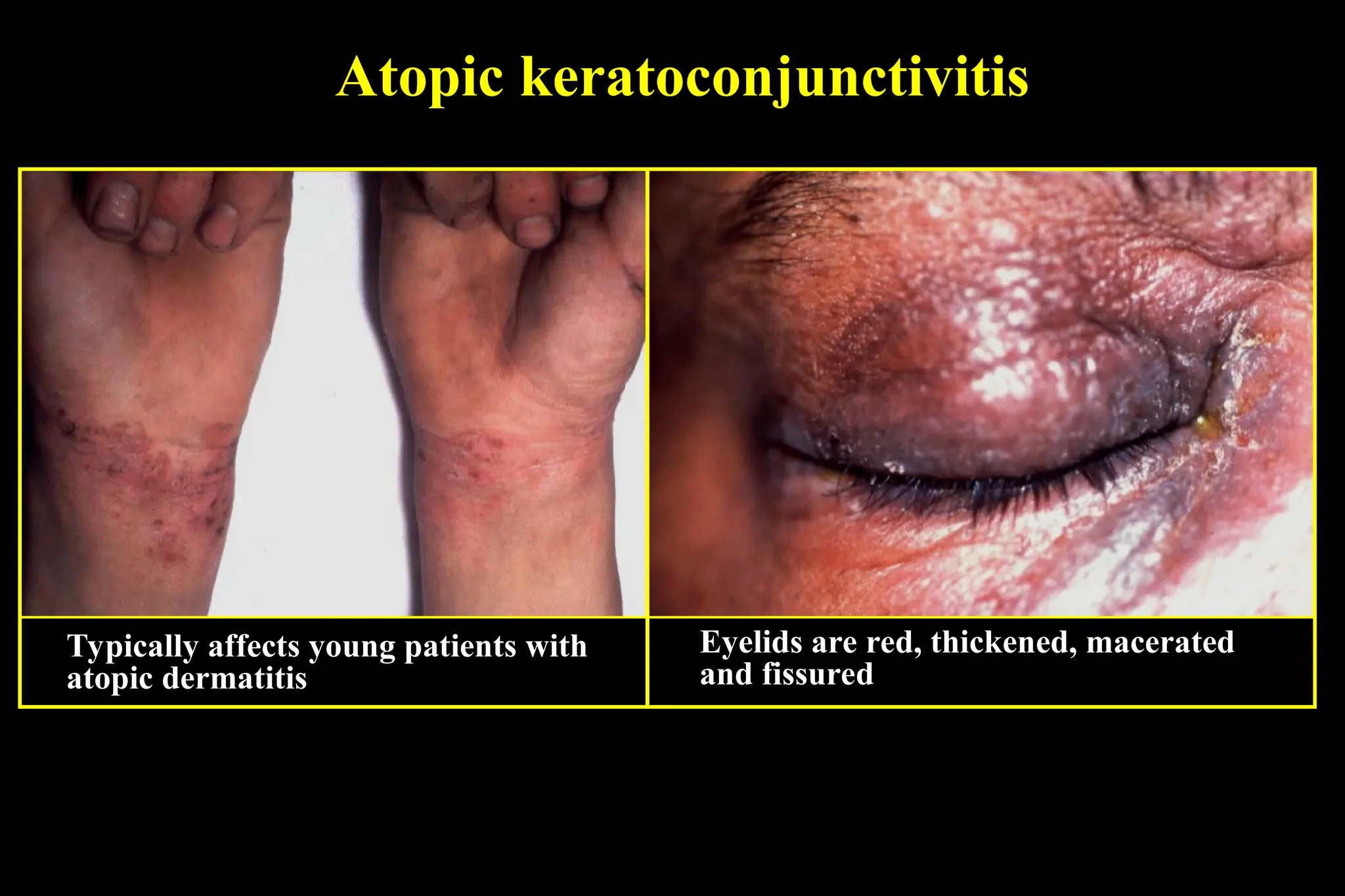
Atopic kertoconjunctivitis
similar toVKC, more severe and unremitting
Rare bilateral
Typically develop in adulthood
No gender preponderance
Tend to be perennial, worst in winter
Treatment of VKCand AKC
management of VKC does not differ substantially
from that of AKC
• less responsive and requires more intensive and
prolonged treatment
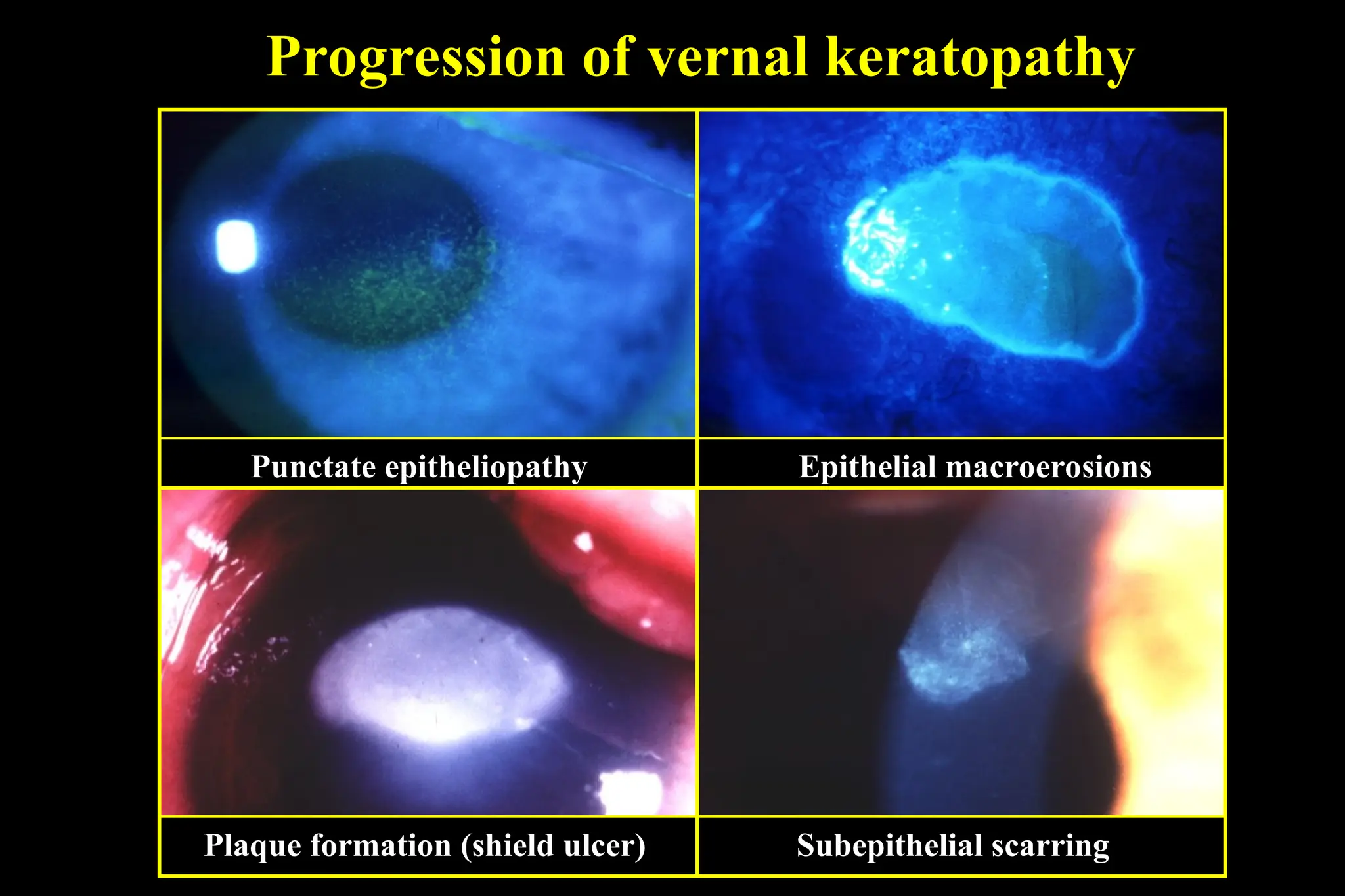
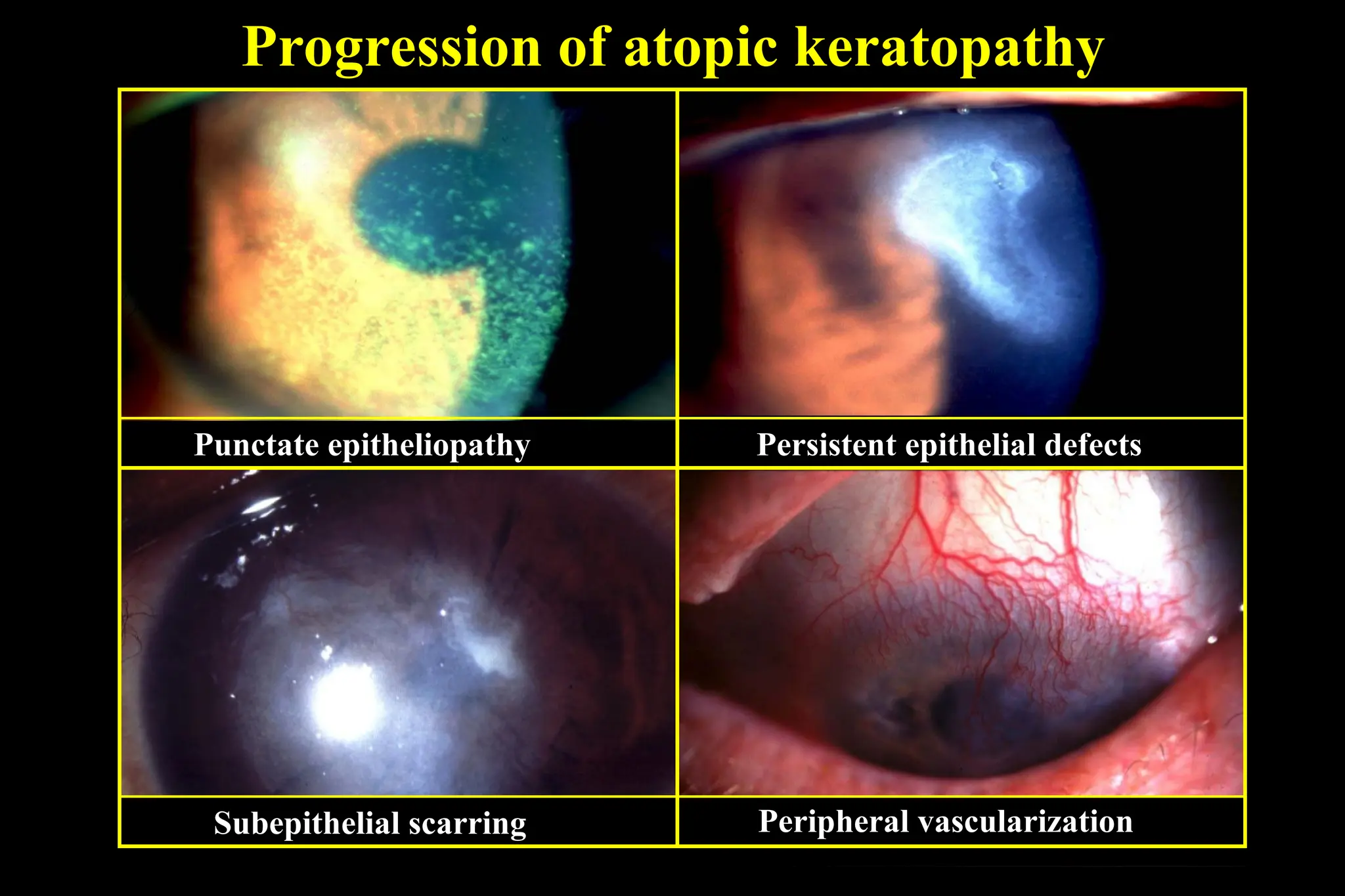
#11 SPK- sheet of mucus on the superior cornea
Epith macroerosion- epithelial toxicity from inflame mediator + direct effect from papillae
Sheild ulcer- exposed Bowman membrane become coat with mucus and calcium phosphate -> inadequate wetting and delayed re-epitheliazation
Scar- grey and oval
#15 SPK- inf 1/3 of cornea
Peripheral Vx- more common than VKC