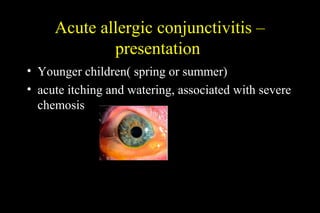
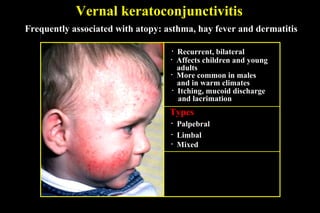
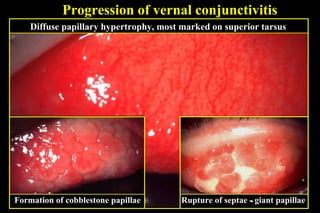
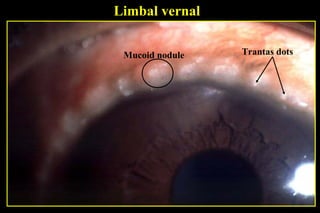
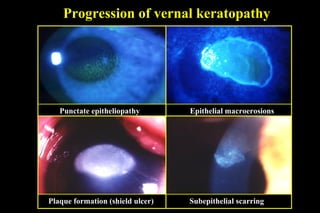
This document discusses different types of allergic eye diseases including acute allergic conjunctivitis, seasonal and perennial allergic conjunctivitis, vernal keratoconjunctivitis (VKC), and atopic keratoconjunctivitis (AKC). It describes the presentation, diagnosis, and treatment of each condition. Acute allergic conjunctivitis commonly affects children and presents as itching and watering. VKC and AKC are chronic, inflammatory conditions that predominantly affect children and young adults. They can progress to involve the cornea and cause scarring if not properly treated with mast cell stabilizers, antihistamines, steroids, and immunosuppressants.