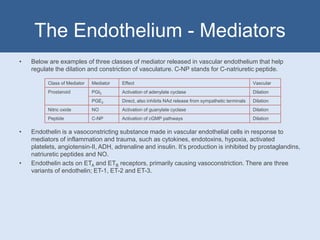
Vasoactive drugs act on vascular smooth muscle to cause vasoconstriction or vasodilation. Vasoconstrictors such as endothelin, angiotensin II, and ADH cause contraction through increasing calcium levels or sensitivity. Vasodilators such as calcium channel blockers, ACE inhibitors, and nitrates cause relaxation through decreasing calcium, increasing cGMP/cAMP, or inhibiting phosphodiesterases. The vascular endothelium releases various mediators like prostanoids, nitric oxide, and C-type natriuretic peptide that regulate vascular tone. RAAS activation leads to vasoconstriction and sodium retention through angiotensin II, while drugs blocking RAAS cause indirect vasodilation.