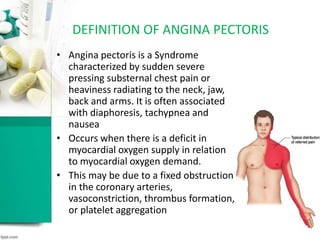
This document provides an overview of nitrates in the management of angina pectoris. It defines angina pectoris and its types, and describes the pathophysiology and rationale for using nitrates. It discusses the class and examples of nitrates, their mechanisms of action, effects, dosages, and interactions. It describes nitrate tolerance and the benefits of nitrate combinations with beta-blockers or calcium channel blockers. In conclusion, the document states that nitrates decrease preload while calcium channel blockers decrease afterload, and beta-blockers decrease heart rate and contractions, making all three drugs beneficial when used together for treating angina.
























































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)



