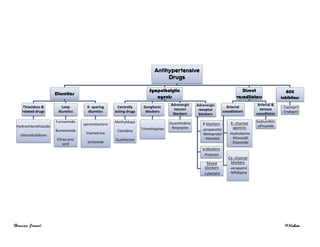
This document summarizes various classes of antihypertensive drugs including diuretics, sympatholytic agents, adrenergic receptor blockers, direct vasodilators, calcium channel blockers, angiotensin converting enzyme inhibitors, and their mechanisms of action, therapeutic uses, and side effects. It also provides guidelines on the management of hypertension including recommendations for first-line drugs for mild or moderate vs. severe hypertension as well as considerations for special populations and hypertensive emergencies.
These are the drugs which antagonize the receptor action of adrenaline and related drugs.
These drugs act by blocking a and/or ß-adrenergic receptors.
α-blockers
PRAZOSIN is a competitive antagonist effective in the management of hypertension. Similar drugs with longer half-lives (e.g. doxazosin, terazosin).
β-blockers
Heart - Decrease heart rate, force of contraction and cardiac output.
Blood Pressure - Decrease in blood pressure (blockage).
Respiratory System – bronchoconstriction.
Eye – Beta-blocking agents reduce intraocular pressure, especially in glaucoma. The mechanism usually reported is decreased aqueous humor production.
Metabolic - Increase LDL and decrease HDL.
Uterus - Relaxation of uterus.
Local anaesthetic - Propranolol has some local anaesthetic action
This presentation contains drugs which blocks the adrenergic system e.g receptor blockers like alpha and beta receptor antagonists, adrenergic neuron blocking agents in details.various animated pictures are also included to make the presentation interesting as well as i have used various diagrams and tables to have better understanding of the topic. Thank you.
Dr. Jibachha Sah,M.V.Sc( Veterinary pharmacology, TU,Nepal),posted lecturer notes on AUTONOMIC AND SYSTEMIC PHARMACOLOGY for B.V.Sc & A.H. 6 th semester veterinary students of College of veterinary science,Nepal Polytechnique Institute, Bharatpur, Bhojard, Chitwan, Nepal.I hope this lecture notes may be beneficial for other Nepalese veterinary students. Please send your comment and suggestion .Email:jibachhashah@gmail.com,moble,00977-9845024121
These are the drugs which antagonize the receptor action of adrenaline and related drugs.
These drugs act by blocking a and/or ß-adrenergic receptors.
α-blockers
PRAZOSIN is a competitive antagonist effective in the management of hypertension. Similar drugs with longer half-lives (e.g. doxazosin, terazosin).
β-blockers
Heart - Decrease heart rate, force of contraction and cardiac output.
Blood Pressure - Decrease in blood pressure (blockage).
Respiratory System – bronchoconstriction.
Eye – Beta-blocking agents reduce intraocular pressure, especially in glaucoma. The mechanism usually reported is decreased aqueous humor production.
Metabolic - Increase LDL and decrease HDL.
Uterus - Relaxation of uterus.
Local anaesthetic - Propranolol has some local anaesthetic action
This presentation contains drugs which blocks the adrenergic system e.g receptor blockers like alpha and beta receptor antagonists, adrenergic neuron blocking agents in details.various animated pictures are also included to make the presentation interesting as well as i have used various diagrams and tables to have better understanding of the topic. Thank you.
Dr. Jibachha Sah,M.V.Sc( Veterinary pharmacology, TU,Nepal),posted lecturer notes on AUTONOMIC AND SYSTEMIC PHARMACOLOGY for B.V.Sc & A.H. 6 th semester veterinary students of College of veterinary science,Nepal Polytechnique Institute, Bharatpur, Bhojard, Chitwan, Nepal.I hope this lecture notes may be beneficial for other Nepalese veterinary students. Please send your comment and suggestion .Email:jibachhashah@gmail.com,moble,00977-9845024121
EFFECTS OF EXCESS SALT DIET ON ANGITENSINOGEN SECRETIONS IN THE KIDNEY OVER TIMEchiehyin
Abstract
Background: Salt is an important component for normal function of cells. However, we consume more than 10 times the salt that is required. This high salt content affects the renin–angiotensin–aldosterone system (RAAS) that regulates blood pressure (BP) and water content of our body. Angiotensinogen is an oligopeptide hormone precursor serving as a substrate for renin in the formation of angiotensin I. Angiotensin I is converted to angiotensin II that causes vasoconstriction and a subsequent increase in BP. We hypothesized that angiotensinogen secretions increases in the kidney and urine with intake of high salt diet.
Methods: Dahl salt sensitive (SS) and salt resistant (SR) male rats (8 weeks old) were fed with high salt (HS) and low salt (LS) diet along with or without aldosterone (ALDO); aldosterone antagonist, eplerenone (EPL); and NADPH oxidase inhibitor, apocynin (APC) for 21 days. Urine samples and kidney were collected; total proteins isolated, and quantified using the microassay procedure and analyzed by western blot for angiotensinogen.
Results: Angiotensinogen was detected in the kidney samples of Dahl SS rat when fed either low or high salt diet, whereas angiotensinogen was detected in kidney samples of Dahl SR rats when fed with high salt diets. Angiotensinogen was not detected in urine samples.
Conclusions: In conclusion, consuming a high salt diet increases Angiotensinogen that lead to an increase in angiotensin II which may cause an increase in BP.
Acknowledgements: Vivien Thomas Summer Research Program, Morehouse School of Medicine, Atlanta, GA, USA.
Basic must know things about Anti Hypertensive drugs including the recent JNC-8 classification and protocols for treating Hypertension with various co-morbid condition.
Antihypertensives | Classes of Drugs | Baro ReceptorChetan Prakash
This Presentation provides a knowledge about Antihypertensives, types of blood pressure, hypertension types, normal blood pressure regulation, baro receptors, classes of antihypertensive drugs,recent discovery on hypertension. This is an assignment for the subject, Advanced Pharmacology-I, 1st year M.Pharm, 1st semester.
2. Diuretics
Diuretics lower BP primary by depleting body Na+
stores.
Na+
increases BV & PVR by: ↑ vessel stiffness & ↑neural reactivity
Thiazides & related drugs Loop diuretics K- sparing diuretics
Mechanism
1) Initial ↓ in blood volume & COP
2) After chronic administration (6-8
weeks), COP gradually returns to
normal while PVR declines due to:
a. Loss of Na+
from arterial wall
b. ↓ sensitivity of vascular or
smooth muscle to NE
1) More potent than thiazides as
diuretics BUT less potent as
antihypertensive
2) The antihypertensive effect of
loop diuretics is related ↓ BV
Indicated in cases of
- Mild or moderate hypertension
(lowering BP by 10-15 mmHg)
- In sever hypertension in
combination with other
antihypertensive drugs
- Hypertension associated with
reduced glomerular filtration rate
(↓ GFR) – Renal impairment
- Heart failure or liver cirrhosis,
where Na retention is marked
- Hypertension in which multiple
drugs with Na retaining properties
are used (Contraceptives)
- Avoid excessive K depletion
particularly in patients taking
digitalis
- Enhance the natriuretic effects
of other duretics
Side effects
1) Hypokalemia (Except for K- sparing diuretics)
2) Impair glucose tolerance, diabetes mellitus and increase serum lipid conc.
3) Impotence loss of libido, diarrhea and gout
3. Sympathetic agents
Centrally acting drugs
Ganglionic blockers
( Symp. & para.)
Adrenergic neuron blockers
Clonidine Methyldopa Trimethaphan Guanethidine Reserpine
Mechanism
1) Central action
stimulates the central
presynaptic α2-receptors
that are inhibitory to
sympathetic outflow
2) Peripheral action
- Reduces the release of NE
from adrenergic nerve
- Prevents cardiac
responses to
postganglionic adrenergic
nerve stimulation
- Has a weak direct
peripheral vasodilation
action
Converted into α-
methyl NE (potent α2-
adrenergic agonist) in
the CNS, this would
lead to decrease in
sympathetic outflow
(M Dopa αM NE
α2 agonist ↓NE
↓Symp.)
1) ↓ sympathetic
vasoconstriction tone
leading to:
a. Dilation of the
arterioles
b.Dilation of the
veins
2) Produces a direct
vasodilation action &
histamine like effect
It inhibits the release
of NE that occur when
a normal action
potential reaches
sympathetic nerve
ending thus tend to
↓COP by bradycardia
and relaxation of
capacitance vessels
- With chronic
therapy, COP
returns to normal
while PVR ↓
- Blocks the ability of
adrenergic
transmitter vesicles
to uptake and store
biogenic amines by
interfering with
uptake mechanism,
resulting in
- Depletion of NE,
Dopamine &
serotonin in both
central and
peripheral vascular
resistance
Therapeutic
uses
- Moderate
Hypertension
- prophylactic
treatment for margin
moderate & sever
forms in hypertension
- In malignant
hypertension
- Acute pulmonary
edema due to
hypertensive cardiac
failure
- Hypertensive
encephalopathy
Little use due to side
effects
Little use due to its
side effects
Side effects
- Sedation & dry mouth
- Postural hypotension
- Rebound hypertension if
clonidine is suddenly
withdrawn
Guanfacine ~ clonidine
-Sedation on long
term therapy
- Impaired mental
concentration &
mental depression
- Nightmares &
vertigo
- Postural hypotension
& Tachycardia
- Constipation, dry
mouth, urinary
retention
- Mydriasis
- Impotence
-Postural
hypotension and
hypotension
following exercise
-Diarrhea and
delayed ejaculation
- Postural
hypotension
- Sedation, nightmars
and severe mental
depression
- Diarrhea and
increase gastric acid
secretion
4. Adrenergic receptor Blockers
Propranolol (β) Metoprolol & Atenolol (β) Prazosin (α) Labetalol (Mixed)
Mechanism
1- β1 β2 antagonists
2- Depresses renin-angiotensin-
aldosterone system by
inhibition of renin production
(β2 effect)
β1- selective blockers, both
have side effects fewer
than propranolol
blocking of α1 receptors in
arterioles and venules
Has a vascular smooth
muscle relaxant effect
- It blocks α & β receptors
, β blocking is
predominant
- Reduces the
sympathetic vascular
resistance without
significant alteration in
HR or COP
- reduces plasma renin
activity
Therapeutic uses
- Lowers BP in mild & moderate
hypertension
- Prevent reflex tachycardia
that often results from
treatment with direct
vasodilators in case of sever
hypertension
For treatment of
hypertensive patients who
suffer from asthma,
diabetes or peripheral
vascular disease
Treatment of severe
hypertension in
combination with other
antihypertensive agents
- Hypertension of
pheochromocytoma
(adrenal gland tumors
that produce xss
adrenalin)
- Hypertensive
emergencies
Side effects
- May increase plasma
triglycerides and decrease
HDL-cholesterol
- Nervousness, Nightmares,
Mental depression and
increase intensity of angina
- Asthma, peripheral vascular
insufficiency and diabetes
- Postural hypotension
and tachycardia are
observed with 1st
dose
- Angina pectoris & fluid
retention
- Drowsiness, headache,
GIT disturbance,
blurred vision, dry
mouth
Similar to non-selective β-
blockers
β blockers ↓BP by ↓COP. With continued treatment COP returns to normal but PVR is reset at lower level and thus BP remains low
Ganglionic Blockers (Trimethaphan)
The depolarizing blockers are not used in hypertension as they cause initial stimulation if the ganglia and thus tend to raise BP at first
The competitive blockers suffer from the disadvantage of that they block both sympathetic and parasympathetic ganglia, with the exception of
trimethaphan, so they have been replaced by drugs which have better selective action an sympathetic tone in the prolonged management of
essential hypertension
5. Direct Vasodilators
Arterial vasodilators
Arterial & venous
vasodilator
K+
channel agonists Ca+
Channel blockers
Na Nitroprusside
Hydralazine & Minoxidil Diazoxide Verapamil & Nifidipine
Mechanism
Relaxation of smooth
muscle of arterioles,
↓systemic vascular
resistance
Effective in long acting
arteriolar dilator
Inhibit Ca+
influx in arterial
smooth muscle leading to
dilation of peripheral
arterioles
Dilates both arterial &
venous vessels, resulting in
↓ PVR and venous return
K+
out, can’t Ca+2
in, relaxation
Therapeutic uses
Out patient’s therapy of
hypertension
hypertensive emergencies
Mild to moderate
hypertension, Angina or
coronary spasm
Hypertensive emergencies
severe cardiac failure
Side effects & toxicity
- ↑ HR & stroke volume
due to compensatory
responses mediated by
baroreceptors and
sympathetic NS as well
as renin and
aldosterone leading to
↑ COP and renal blood
fllow
- Tachycardia, palpitation
and angina
- Headache, nausea,
anorexia, sweating and
flushing
- Excessive hypotension
with tachycardia and ↑
COP
- Hyperglycemia due to
the inhibition of insulin
release
- Salt & water retention
Slight tachycardia & in ↑
COP
Prolonged therapy leads to
accumulation of: CN-
/ SCN-
1) Cyanide (metabolic
acidosis, arrhythmias,
excessive hypotension
& death)
2) Thiocyanate
(weakness, psychosis,
muscle spasm &
cconvulsion
Both can be avoided by:
Sodium thiosulfate as a
sulfur donor or hydroxyl
cobolamin
Nausea, vomiting,
sweating, restlessness,
headache and palpitation
6. Angiotensin converting enzyme inhibitors
(Captopril – Enalapril)
Action by renin-angiotensin –
aldosterol system
Angiotensin
𝑅𝑒𝑛𝑖𝑛 𝑟𝑒𝑙𝑒𝑎𝑠𝑒𝑑 𝑓𝑟𝑜𝑚 𝑟𝑒𝑛𝑎𝑙 𝑐𝑜𝑟𝑡𝑒𝑥
�⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯� Angiotensin I
𝑖𝑛 𝑡ℎ𝑒 𝑙𝑢𝑛𝑔 𝑏𝑦 𝐴𝐶𝐸
�⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯� Angiotensin II
𝑖𝑛 𝑡ℎ𝑒 𝑎𝑑𝑟𝑒𝑛𝑎𝑙 𝑔𝑙𝑎𝑛𝑑
�⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯⎯� Angiotensin III
- Angiotensin II has a vasoconstrictor and Na retaining activity
- Booth Angiotensin II & Angiotensin III stimulate aldosterone release, which increase Na and water retention
and thus the blood pressure increase
Mechanism
- Inhibit the ACE and thus inhibit the action of renin- angiotensin- aldosterone system
- They stimulate Kallikrein-Kinin system (bradykinin) which has a potent vasodilation effect.
- The hypotensive effect of ACE inhibitor is associated with increasing glomerular filtration rate
Therapeutics
Treatment of:
- sever or refractory hypertension -Hypertensive diabetic patients
- Renal insufficiency to increase glomerular filtration rate
Side effects - Proteinuria - Neutropenia or Pancytopenia - Skin rashes, drug fever, taste impairment and dry cough