Ε. ΑΝΔΡΙΩΣΗ
Ο ρόλοστησ ακτινοθεραπείασ ςτον
καρκίνο του προςτάτη
1ο Συμπόσιο Κλινικής Ογκολογίας Ρόδου
Ακτινοθεραπευτήσ Ογκολόγοσ
Euromedica – Αθήναιον Α & Ιατρικό Κέντρο Αθηνών
2.
Δηλώνω ότι δενζχω
(προςωπικά ή ωσ μζλοσ εργαςιακήσ/ερευνητικήσ ομάδασ) ή μζλοσ τησ
οικογζνειάσ μου οποιοδήποτε οικονομικό ή άλλου είδους όφελος από τισ
εταιρείεσ/επιχειρήςεισ που διοργανώνουν /χρηματοδοτοφν την άνω
εκδήλωςη κατά τη διάρκεια των τελευταίων 4 ετών.
Χορηγοί Εταιρείεσ
AMGEN
ARITI
ASTRA
GALENICA
GENESIS
PHARMAZAC
ROCHE
SANOFI AVENTIS
PFIZER
TEVA
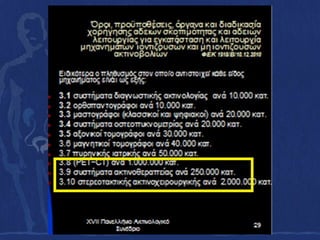
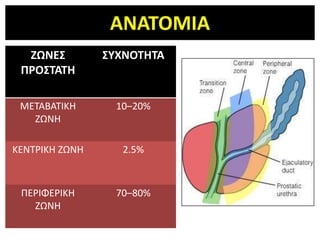
ΜΟΝΑΓΑ ΜΔΣΡΗΗ ΑΚΣΙΝΟΘΔΡΑΠΔΙΑ
Dose is the amount of radiation used to treat
a patient
SI unit (joules/kg)
Gray (Gy)
Centigray (cGy)
100 cGy = 1 Gy
Similar to milligrams for drugs
180 cGy or 200 cGy per day or 1.8 Gy or 2
Gy per day is usually given to treat prostate
1.8 Gy x 42 treatments = 75.6 Gy total
Treatment options
T1/T2 disease
• The standard approaches for men with organ-confined
T1/T2 prostate cancer are
– radical prostatectomy (RP)
– external beam radiation therapy (EBRT),
– brachytherapy, and
– active surveillance
For patients receiving definitive treatment for T1/T2
prostate cancer, the choice of therapy is largely a matter
of patient preference. There is no evidence that the cure
rate is different with RP, EBRT, or brachytherapy when
patients are stratified based upon prognostic
characteristics
44.
Intermediate- or high-risk
•Intermediate-risk disease
EBRT, brachytherapy, or RP
• High-risk disease
ADT plus EBRT or RP plus adjuvant EBRT
Σςσαιοποιημένερ μελέηερ ποςδείσνοςν ηο όθελορ από ηην
αύξηζη ηηρ δόζηρ (συπίρ IMRT και οπμονοθεπαπεία)
RCT N Comparison Result
Pollack 301 70Gy/35 vs. 78Gy/39 59% vs. 78% bPFS at
(MDA) 5 years
2007 update
Zietman 393 70.2Gy vs. 79.2Gy (proton boost) 61% vs. 80% bPFS at
2005 5 years
Peeters 664 68Gy/34 vs. 78Gy/39 54% vs. 64% FFF at 5
(Dutch) years
2006
Dearnaley 843 64Gy/32 vs. 74Gy/37 60% vs. 71% bPFS at
(RTO1) 5 years
2007
Hoskin 220 55Gy/20 vs. 35.75Gy/13 + HDR 8.5Gy x 2 64% vs. 80% bPFS at
(Mt Vernon) 5 years
2007
bPFS=biochemical progression free survival FFF= freedom from failure
59.
Prostate Cures Ratesby Treatment and Dose
External beam > 72Gy
Surgery or Seeds
External beam < 72Gy
IJROBP 2004; 58:25
Months
60.
Improving the Resultsof Radiotherapy
Dose escalation– increasing the dose of
radiation by 10% can increase local control
by 20%
3D Conformal, IMRT, HDR Brachytherapy boost
Combination treatment with radiotherapy and
androgen suppression
IMRT (intensity
modulated
radiation therapy)
using 7 different beams
to target the prostate
The computer can
determine the optimal
number of beams to
deliver the radiation
dose to hit the target and
avoid other structures
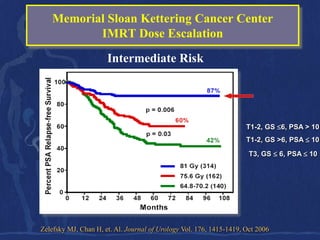
Memorial Sloan KetteringCancer Center
IMRT Dose Escalation
• Began using IMRT in 1996 to facilitate dose
escalation
• high dose XRT using IMRT for localized prostate
cancer
• 561pts. B/w April 1996 & Jan 2000
• Median age 68 (range 46-86)
Zelefsky MJ, Chan H, et. Al. Journal of Urology Vol. 176, 1415-1419, Oct 2006
69.
Memorial Sloan KetteringCancer Center
IMRT Dose Escalation
Low Risk
T1-2, GS ≤6, PSA ≤10
Zelefsky MJ, Chan H, et. Al. Journal of Urology Vol. 176, 1415-1419, Oct 2006
Memorial Sloan KetteringCancer Center
IMRT Dose Escalation
High Risk
GS >6, PSA >10
Zelefsky MJ, Chan H, et. Al. Journal of Urology Vol. 176, 1415-1419, Oct 2006
72.
Memorial Sloan KetteringCancer Center
IMRT Dose Escalation
Biochemical Control
• Using the ASTRO definition, the 8-year actuarial PSA
relapse-free survival
– Favorable risk: 85%
– Intermediate risk: 76%
– Unfavorable risk: 72%
Zelefsky MJ, Chan H, et. Al. Journal of Urology Vol. 176, 1415-1419, Oct 2006
73.
Loma Linda ProtonBeam Experience
Dose Escalation
.
• B/w Oct 1991 & Dec 1997,
• 1255 pts with Stages Ia-III prostate cancer
• No prior surgery, hormonal therapy, or distant
mets
• Treated with protons alone or in combination with
photon-beam XRT
Slater JD, Rossi CJ, et. Al. IJROBP Vol 59, No. 2, 348-352, 2004.
75.
There is significantmovement of the prostate gland
based on daily gas in rectum
Planned
target
No Rectal
gas
Planned target,
missed badly if
rectal gas pushes
the prostate Rectal gas
forward
76.
Image Guided RT(IGRT)
• ALL MODERN RT DELIVERY SHOULD BE IGRT
• Improve accuracy of treatment
• Track daily position of the prostate before delivering RT
• Fiducial markers (x-rays), ultrasound scans, electromagnetic
tracking, CT scans (cone beam CT, fiducials), endorectal
balloon (x-rays, CT scan)
The most sophisticatedtechnique for image
guided IMRT is Tomotherapy.
Combine a CT scan and linear accelerator to ultimate in
targeting (IGRT) and ultimate in delivery (dynamic, helical
IMRT) ability to daily adjust the beam (ART or adaptive
radiotherapy)
Better Cure Rateswith Image Guided IMRT
compared to IMRT for Prostate
Intermediate Risk High Risk
82.
Lower Risk ofSide Effects with Image Guided IMRT
compared to IMRT
83.
CHHiP Trial
• Conventionalor Hypofractionated High Dose
Intensity Modulated Radiotherapy for Prostate
Cancer
• Hypothesis: hypofractionated radiotherapy
schedules for localised prostate cancer will
improve the therapeutic ratio by either:
a) Improving tumour control
b) Reducing normal tissue side effects
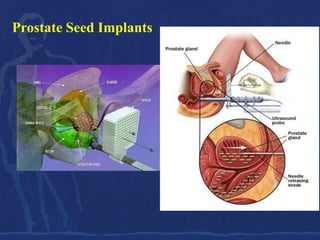
ΔΜΦΤΣΔΤΗ ΚΟΚΚΩΝ
• The implant is done under general
anesthesia in OR.
• Radioactive seeds are implanted into
the prostate gland under transrectal
ultrasound guidance, using needles
that pass through the skin between the
legs behind the scrotum (the
perineum).
• Each needle may deliver between 2-6
seeds and, usually, 20-30 needles are
required to implant 80-140 seeds.
• The seeds are woven into a strand of
absorbable material to help maintain
their position and reduce the risk of
seed migration.
• The procedure takes about 90 minutes
and after recovery the patient can go
home.
HDR Brachytherapy PlusEBRT
• 1260 patients with a PSA >10 ng/mL, GS >7 or
>cT2b from 3 institutions
• EBRT to pelvis or prostate + HDR brachytherapy*
– EBRT: 36-50 Gy + 1.8-2 Gy daily 5x per week
– HDR brachytherapy: dose escalated from 5.5 Gy x 3
to 15 Gy x 2
• At 4.4-years’ median follow-up, 8-year bNED
was 81% Martinez et al 2005
HDR, high dose rate
*Usually done with high activity iridium-192 (10 Ci sources);
106.
AMERICAN BRACHYTHERAPY AMERICAN BRACHYTHERAPY
SOCIETY SOCIETY
PROSTATE HIGH-DOSE RATE PROSTATE LOW-DOSE RATE
TASK GROUP TASK GROUP
I-Chow Hsu, MD, Yoshiya Yamada MD, Eric Vigneault MD, Jean Gregory S. Merrick, M.D., Michael J. Zelefsky, M.D., John
Pouliot, PhD August, 2008 Sylvester, M.D., Subir Nag, M.D., William Bice, Ph.D.
Doses
Monotherapy
Pd-103
125 Gy (110-120 Gy)
10.5 Gy x 3
I-125
8.5-9.5 Gy x 4
145 Gy (140-160 Gy)
6.0-7.5 Gy x 6
Cs-131
115 Gy
BT + EBRT
Pd-103
15 Gy x 1 (with 36-40 Gy XRT) Boost (with 41.4 – 50.4 Gy EBRT)
9.5-10.5 Gy x 2 (with 40-50 Gy XRT) 90-100 Gy
5.5-7.5 Gy x 3 (with 40-50 Gy XRT) I-125
4.0-6.0 Gy x 4 (with 36-50 Gy XRT) Boost (with 41.4 – 50.4 Gy EBRT)
108-110 Gy
ΤΜΠΔΡΑΜΑΣΑ
• LDR SEEDSgold standard for prostate
brachytherapy in low risk patients
• HDR BOOST effective dose escalation in
intermediate and high risk patients
• HDR monotherapy still experimental
EORTC 22863 at5.5 years’
Median Follow-up
100
80
Patients
surviving
60
(%)
40
HR 0.51 (95% CI 0.36, 0.73; p<0.001)
20 Goserelin + RT (n=207)
RT alone (n=208)
0
0 1 2 3 4 5 6 7 8
Time since randomisation (years)
Bolla et al 2002
T1-2 of WHO grade 3 or T3-4 N0-1, M0 disease
114.
Bicalutamide Adjuvant toRadiotherapy
Significantly Improves Survival
Locally advanced disease at 7.4 years’ median follow-up
100
Total deaths
Prostate cancer-specific deaths
80
HR 0.65 In the RT group,
60 (p=0.03) numerically fewer
Mortality
patients receiving
(%)
40 bicalutamide died due to
prostate cancer vs.
placebo (16.1% vs.
20
24.3%)
0
Bicalutamide Radiotherapy
+ radiotherapy alone
115.
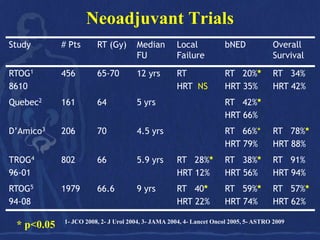
Adjuvant Hormonal Therapy
•4 randomized trials
– RTOG 85-31 Pilepich et al. IJROBP 2005
– EORTC 22863 Bolla et al. Lancet 2002
– RTOG 92-02 Horwitz et al. JCO 2008
– Quebec L-200 Laverdiere et al. J Urol 2004
• Higher risk patients
– Mixed population
• T stage
• Post-op
• N positive
• Low/Intermediate Risk
Combination Therapy asan Adjuvant to
Radiotherapy: Clinical Trials
Significant improvement in Bolla et al, 1997, 1999, 2002
overall and disease-free survival EORTC 22863
Significant improvement in Pilepich et al, 1997, 2003
disease-free survival Lawton et al, 1999
Significant improvement in RTOG 85-31
overall survival (patients with
Gleason scores 8–10)
Significant improvement in Hanks et al, 2000
disease-free survival, local RTOG 92-02
progression, distant metastases
and biochemical progression
EORTC, European Organisation for Research and Treatment of Cancer
118.
Harvard Study: Adding6 months of hormones to RT
improved survival in intermediate-risk and high-risk disease
Intermediate-risk High-risk
IJROBP 2010
119.
Harvard Study
• Allpatients were treated with ADT for 6 months (combined
androgen blockade) along with external beam radiotherapy and then
randomized to either 30 further months of ADT (LHRH agonist
monotherapy) or no further ADT.
• The study was designed to show non-inferiority between short-term
and-long term ADT.
• The study was stopped at a preplanned interim analysis.
• Long-term ADT significantly increased 5-year biochemical PFS
(78.3% vs 58.9%), 5-year clinical PFS (81.8% vs 68.9%) and 5-year
overall survival (85.3% vs 80.6%) in this patient population.
• This study’s conclusions support the previous EORTC study
published by Bolla et al (NEJM 1997, Lancet 2002) showing a
benefit with 3 years of ADT in patients with locally advanced prostate
cancer treated with external beam radiotherapy.
120.
Short vs. long*adjuvant ADT after RT
*3 years vs. 6 months
Overall survival
Bolla et al., ASCO 2007
121.
RT + HormonalTherapy
Summary
• Prolonged use of hormonal therapy beneficial for high risk
patients
• Short use of hormonal therapy appears beneficial for
intermediate risk
• Optimal duration of hormonal therapy still unknown
• Toxicity is increased
• Health costs is an issue
• Closed studies
– 36 months vs 6 months (EORTC)
– 36 months vs 18 months (Quebec)
122.
Locally Advanced ProstateCancer: A clinical
dilemma that has not gone away
Multimodality therapy is the standard of
care for these patients
• EBRT/ADT
• Surgery/adjuvant radiotherapy
Side Effects ofProstate Radiation
Radiation
zone
The structures that will get hit by radiation
and have inflammation or irritation:
bladder, urethra and rectum
138.
Radiation
zone
Short Term Side Effects:
Irritation of bladder, urethra
and rectum
1. Urinary frequency (getting up at night very few hours,
take NSAID’s, or may benefit from medication)
2. Slight burning or stinging with urination (drink cranberry
juice)
3. Diarrhea or more frequent, softer bowel movements,
rectal soreness (take Imodium)
4. Mild skin irritation is now rarely seen
5. Fatigue is common
139.
Radiation
zone
Long Term Side Effects:
Irritation of bladder,
urethra and rectum
Chronic radiation cystitis or proctitis: about 6% of the men
will have occasional episodes of blood in the urine or with
bowel movements, this usually responds to medication (e.g.
cortisone suppositories) The risk of serious damage to the
bladder and rectum is now less than 1%
Impotence: about 30% of men have problems after radiation
140.
Quality of Life/ Medicare Survey
Prostate Cancer Patients
Symptom Surgery Radiation
Wear Pads 30% 7%
Potent (< 70y) 11% 33%
Potent (>70y) 12% 27%
More frequent bowel 3% 10%
movements
J Clin Oncol 14 (8): 2258-65, 1996



















![Roach formulas
Percentage risk of ECE 3/2 PSA + [(GS - 3) x 10]
Percentage risk of SVI PSA + [(GS - 6) x 10]
Percentage risk of LN involvement 2/3 PSA + [(GS - 6) x 10]
Roach III, J Urol 1993;150:1923](https://image.slidesharecdn.com/vakalis-prostate-130331133437-phpapp01/85/Vakalis-prostate-22-320.jpg)

![ΚΑΡΚΙΝΟ ΣΟΤ ΠΡΟΣΑΣΗ: ΑΚΣΙΝΟΘΕΡΑΠΕΙΑ
ΑΚΣΙΝΟΒΟΛΗΗ ΠΤΕΛΟΤ
ΥΠΟΛΟΓΙΣΜΟΣ ΚΙΝΔΥΝΟΥ ΜΕΤΑΣΤΑΣΕΩΝ ΣΤΟΥΣ ΠΥΕΛΙΚΟΥΣ ΛΕΜΦΑΔΕΝΕΣ
1. Αλγόριθμος ηοσ Roach: +LN = 2/3 PSA + [(GS-6) x 10]
2. Πίνακες ηοσ Partin:
T2c
GS=7
PSA=4-6 +LN
16%](https://image.slidesharecdn.com/vakalis-prostate-130331133437-phpapp01/85/Vakalis-prostate-24-320.jpg)