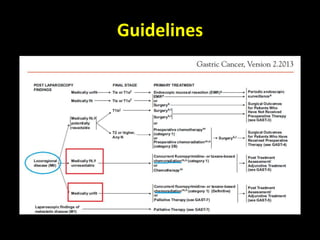
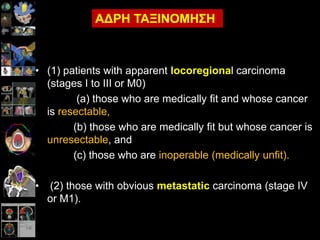
• (1) patientswith apparent locoregional carcinoma
(stages I to III or M0)
(a) those who are medically fit and whose cancer
is resectable,
(b) those who are medically fit but whose cancer is
unresectable, and
(c) those who are inoperable (medically unfit).
• (2) those with obvious metastatic carcinoma (stage IV
or M1).
ΑΔΡΗ ΣΑΞΙΝΟΜΗΗ
Καξθίλνο ηνπ ζηνκάρνπ
πκπιεξσκαηηθήΑθηηλνζεξαπεία
• British Stomach Cancer Group (1994):
– N = 436, ηάδην II – III [N = 63 (14%) κε ππνιεηπόκελε λόζν]
– Όινη νη αζζελείο ππεβιήζεζαλ ζε γαζηξεθηνκή .
– 3 ζθέιε: γαζηξεθηνκή vs +ΑΚΘ vs +ΥΜΘ.
– ΑΚΘ: 4500/25 ± 500cGy boost (Ζεύγνο πξνζζην-νπίζζησλ πεδίσλ)
– ΧΜΘ: MAF x 8 .
• Σνπηθή ππνηξνπή (12 κήλεο): 26% vs 9% vs 15%
Σν εύξνο ηεο δηαθνξάο δελ επαλαιακβάλεηαη ζηνπο
60 κήλεο
• 5-εηή επηβίσζε: 20% v 12% v 19% (NS).
Hallissey MT et al. The second British Stomach Cancer Group trial of
adjuvant radiotherapy Or chemotherapy in resectable gastric cancer: five-
year follow-up. Lancet 1994;343:1309-12.
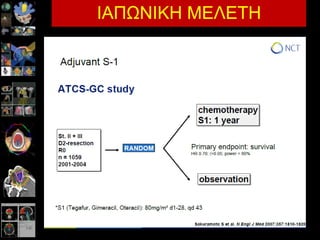
Surgically (D2)
resected StageII,
IIIA, or IIIB GC,
6 weeks prior to
randomization
No prior
chemotherapy or
radiotherapy
n=1035
Capecitabine: 1,000mg/m2 bid, d1–14, q3w
Oxaliplatin: 130mg/m2, d1, q3w
R
A
N
D
O
M
I
Z
A
T
I
O
N
1:1
†
n=520
n=515
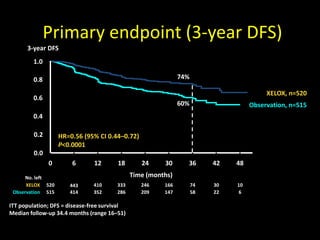
• Primary endpoint: 3-year DFS‡
• Secondary endpoints: overall survival and safety profile
†Stratified by stage and country with age, sex, and nodal status as covariates
‡GASTRIC project: 3-year DFS and 5-year overall survival are strongly associated,
Burzykowski et al. ASCO 2009
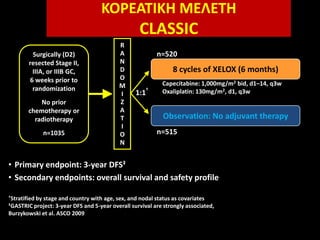
ΚΟΡΕΑΣΙΚΗ ΜΕΛΕΣΗ
CLASSIC
8 cycles of XELOX (6 months)
Observation: No adjuvant therapy
Stomach Cancer Adjuvant
Multi-institutionalTrial
(Samit) trial.
2x2 factorial randomized phase III trial to investigate
weekly paclitaxel (PTX) followed by oral
fluoropyrimidines (FPs) versus FPs alone as adjuvant
chemotherapy in patients (pts) with gastric cancer.
R
A
N
D
O
M
Observation
5FU/LV Radiation
5FU/LV
5FU/LVX2
45Gy/25d
281 pts
275pts
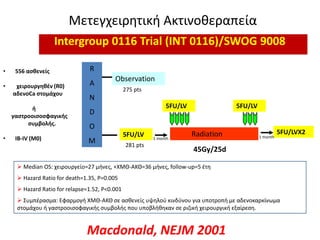
Μετεγχειρθτικι Ακτινοκεραπεία
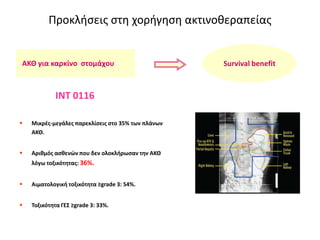
Intergroup 0116 Trial (INT 0116)/SWOG 9008
• 556 αςθενείσ
• χειρουργηθζν (R0)
αδενοCa ςτομάχου
ή
γαςτροοιςοςφαγικήσ
ςυμβολήσ.
• IB-IV (M0)
5FU/LV
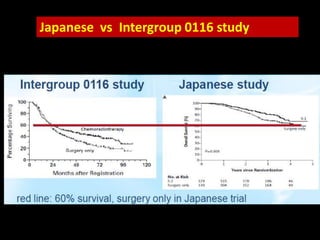
Median OS: χειρουργείο=27 μινεσ, +ΧΜΘ-ΑΚΘ=36 μινεσ, follow-up=5 ζτθ
Hazard Ratio for death=1.35, P=0.005
Hazard Ratio for relapse=1.52, P<0.001
υμπζραςμα: Εφαρμογι ΧΜΘ-ΑΚΘ ςε αςκενείσ υψθλοφ κινδφνου για υποτροπι με αδενοκαρκίνωμα
ςτομάχου ι γαςτροοιςοφαγικισ ςυμβολισ που υποβλικθκαν ςε ριηικι χειρουργικι εξαίρεςθ.
1 month 1 month
Macdonald, NEJM 2001
23.
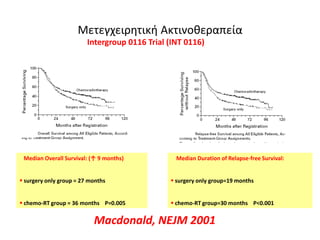
Μετεγχειρθτικι Ακτινοκεραπεία
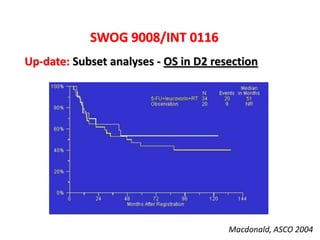
Intergroup 0116Trial (INT 0116)
Median Overall Survival: (↑ 9 months)
surgery only group = 27 months
chemo-RT group = 36 months P=0.005
Median Duration of Relapse-free Survival:
surgery only group=19 months
chemo-RT group=30 months P<0.001
Macdonald, NEJM 2001
24.
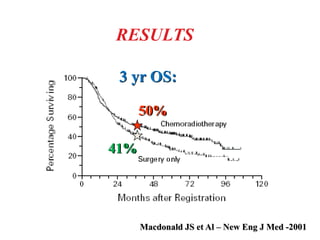
Macdonald JS etAl – New Eng J Med -2001
RESULTS
41% 50%
3 yr OS:
41%
HeCOG, Greece (2002-2005)
adjuvantTaxol/Carbo chemotherapy with or without
radiation therapy
Conclusion: Addition of RT to chemo did not
improve outcomes
Adjuvant chemo vs Adjuvant chemo-RT
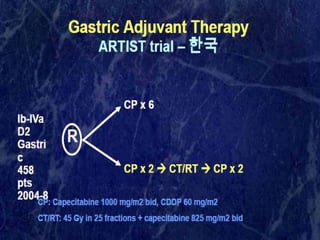
ARTIST
39.
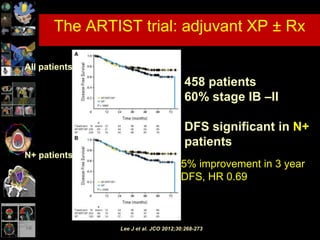
Lee J etal. JCO 2012;30:268-273
The ARTIST trial: adjuvant XP ± Rx
All patients
N+ patients
458 patients
60% stage IB –II
DFS significant in N+
patients
5% improvement in 3 year
DFS, HR 0.69
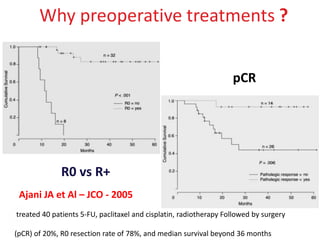
Ajani JA etAl – JCO - 2005
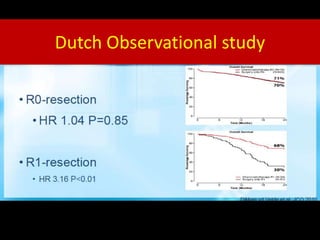
R0 vs R+
pCR
Why preoperative treatments ?
treated 40 patients 5-FU, paclitaxel and cisplatin, radiotherapy Followed by surgery
(pCR) of 20%, R0 resection rate of 78%, and median survival beyond 36 months
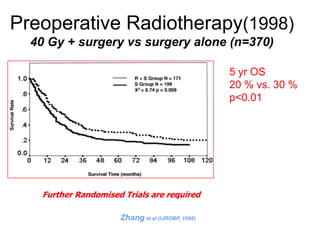
Preoperative Radiotherapy(1998)
40 Gy+ surgery vs surgery alone (n=370)
5 yr OS
20 % vs. 30 %
p<0.01
Zhang et al (IJROBP, 1998)
Further Randomised Trials are required
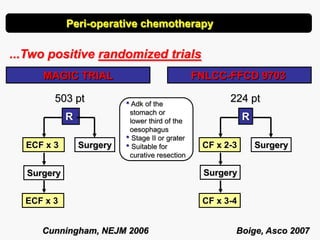
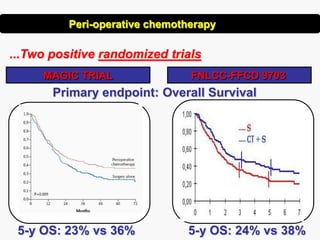
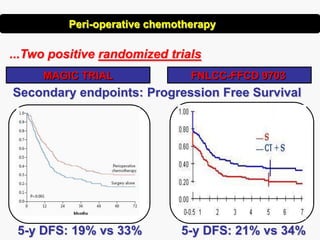
Peri-operative chemotherapy
...Two positiverandomized trials
FNLCC-FFCD 9703MAGIC TRIAL
R R
Surgery SurgeryCF x 2-3
Surgery
CF x 3-4
224 pt503 pt
ECF x 3
Surgery
ECF x 3
Boige, Asco 2007Cunningham, NEJM 2006
• Adk of the
stomach or
lower third of the
oesophagus
• Stage II or grater
• Suitable for
curative resection
...Two positive randomizedtrials
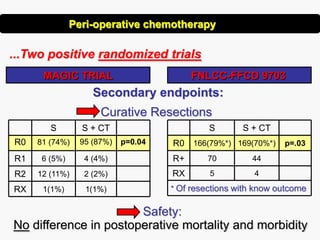
MAGIC TRIAL FNLCC-FFCD 9703
Secondary endpoints:
Curative Resections
Safety:
No difference in postoperative mortality and morbidity
4
44
169(70%*)
S + CT
* Of resections with know outcome
5RX
70R+
p=.03166(79%*)R0
S
1(1%)
2 (2%)
4 (4%)
95 (87%)
S + CT
1(1%)RX
12 (11%)R2
6 (5%)R1
p=0.0481 (74%)R0
S
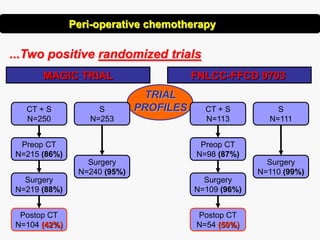
Peri-operative chemotherapy
59.
...Two positive randomizedtrials
CT + S
N=113
Surgery
N=109 (96%)
Preop CT
N=98 (87%)
Postop CT
N=54 (50%)
S
N=111
Surgery
N=110 (99%)
Surgery
N=240 (95%)
S
N=253
CT + S
N=250
Preop CT
N=215 (86%)
Surgery
N=219 (88%)
Postop CT
N=104 (42%)
TRIAL
PROFILES
MAGIC TRIAL FNLCC-FFCD 9703
Peri-operative chemotherapy
60.
Magic Trial
Conclusions
Perioperative chemotherapyin resectable
carcinoma of the stomach and distal esophagus
results in:
• Tumor downsizing and downstaging ?
• Increased PFS
• Increased OS
Peri-operative Chemo is now standard of care in Europe
Πξνεγρεηξεηηθή αθηηλνζεξαπεία
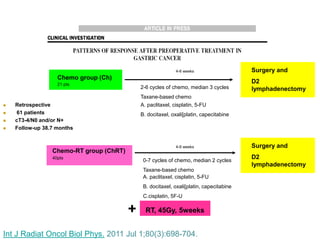
Retrospective
61 patients
cT3-4/N0 and/or N+
Follow-up 38.7 months
Chemo group (Ch)
21 pts
Chemo-RT group (ChRT)
40pts
4-6 weeks Surgery and
D2
lymphadenectomy
A. paclitaxel, cisplatin, 5-FU
B. docitaxel, oxali[platin, capecitabine
2-6 cycles of chemo, median 3 cycles
Taxane-based chemo
Surgery and
D2
lymphadenectomy
4-6 weeks
0-7 cycles of chemo, median 2 cycles
Taxane-based chemo
A. paclitaxel, cisplatin, 5-FU
B. docitaxel, oxali[platin, capecitabine
C.cisplatin, 5F-U
RT, 45Gy, 5weeks+
Int J Radiat Oncol Biol Phys. 2011 Jul 1;80(3):698-704.
66.
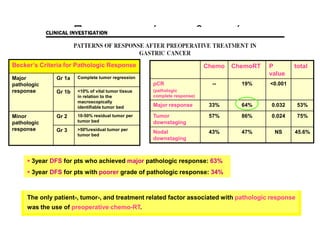
Πξνεγρεηξεηηθή αθηηλνζεξαπεία
Becker’s Criteriafor Pathologic Response
Major
pathologic
response
Gr 1a Complete tumor regression
Gr 1b <10% of vital tumor tissue
in relation to the
macroscopically
identifiable tumor bed
Minor
pathologic
response
Gr 2 10-50% residual tumor per
tumor bed
Gr 3 >50%residual tumor per
tumor bed
Chemo ChemoRT P
value
total
pCR
(pathologic
complete response)
-- 19% <0.001
Major response 33% 64% 0.032 53%
Tumor
downstaging
57% 86% 0.024 75%
Nodal
downstaging
43% 47% NS 45.6%
The only patient-, tumor-, and treatment related factor associated with pathologic response
was the use of preoperative chemo-RT.
3year DFS for pts who achieved major pathologic response: 63%
3year DFS for pts with poorer grade of pathologic response: 34%
67.
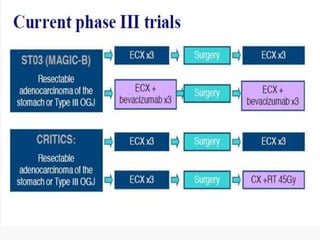
RTOG 99-04
Two phaseII studies from
the M. D. Anderson Cancer
Center
pCR in 26%, R0 resection in 77% MS 23 months, 1yr OS 72%
Multidisciplinary approach forthe
cure of localised gastric cancer
Conclusions
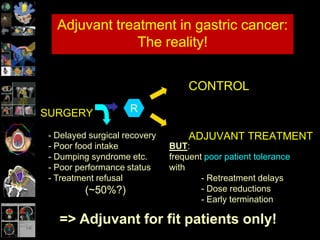
• Adjuvant treatment is efficient but cumbersome and badly
tolerated after gastrectomy
• The role of XRT in (neo)adjuvant TTT of gastric cancer is
still unclear
• Peri-operative or neoadjuvant chemotherapy are better
tolerated and leave less patients behind
• We needed huge meta-analyses to be convinced of
adjuvant therapy while only few studies were sufficient for
the peri-operative strategy!
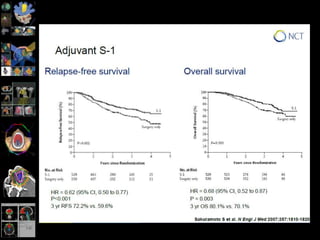
#17 Given this context, we randomized stage II and stage III patients into 2 arms. We compared 8 cycles of Xelox with observation. Most recently, the Korean phase III CLASSIC study reported a significant benefit in DFS from adjuvant combination chemotherapy. Following D2 resection, patients with stage II-IIIb gastric cancer were randomly assigned to eight cycles of adjuvant capecitabine and oxaliplatin (CAPOX) or to observation alone. This positive study shows that a 6-month course of CAPOX after D2 gastrectomy improves 3 year DFS compared with surgery only (74% vs. 59%; p < 0.0001). Chemotherapy reduced the relative risk of disease recurrence, new disease occurrence, or death compared with surgery alone. The OS data are not yet mature; however, the data suggest an improvement in OS with capecitabine and oxaliplatin compared with surgery only (83% vs. 78%; p = 0.0493).10 An analysis after a median follow-up of 5 years is planned to conclusively establish the OS benefit of capecitabine and oxaliplatin in this setting.




![Καξθίλνο ηνπ ζηνκάρνπ
πκπιεξσκαηηθή Αθηηλνζεξαπεία
• British Stomach Cancer Group (1994):
– N = 436, ηάδην II – III [N = 63 (14%) κε ππνιεηπόκελε λόζν]
– Όινη νη αζζελείο ππεβιήζεζαλ ζε γαζηξεθηνκή .
– 3 ζθέιε: γαζηξεθηνκή vs +ΑΚΘ vs +ΥΜΘ.
– ΑΚΘ: 4500/25 ± 500cGy boost (Ζεύγνο πξνζζην-νπίζζησλ πεδίσλ)
– ΧΜΘ: MAF x 8 .
• Σνπηθή ππνηξνπή (12 κήλεο): 26% vs 9% vs 15%
Σν εύξνο ηεο δηαθνξάο δελ επαλαιακβάλεηαη ζηνπο
60 κήλεο
• 5-εηή επηβίσζε: 20% v 12% v 19% (NS).
Hallissey MT et al. The second British Stomach Cancer Group trial of
adjuvant radiotherapy Or chemotherapy in resectable gastric cancer: five-
year follow-up. Lancet 1994;343:1309-12.](https://image.slidesharecdn.com/vakalis-gastric-130615065322-phpapp01/85/Vakalis-gastric-ca-radiotherapy-8-320.jpg)