Downloaded 76 times


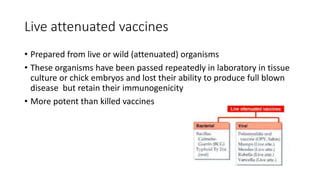





This document summarizes key information about vaccines and immunity: 1. It describes active and passive immunity and how vaccines work to stimulate active immunity through antibody production. 2. It explains herd immunity and how widespread vaccination benefits unvaccinated individuals by making disease transmission unlikely. 3. It provides an overview of different types of vaccines including live attenuated, killed/inactivated, toxoid/subunit, and recombinant vaccines. 4. Examples are given of specific vaccines for diseases like tuberculosis, typhoid, cholera, pertussis, polio, rabies, hepatitis B, and measles/mumps/rubella.






![Vaccines [pharmacy]](https://cdn.slidesharecdn.com/ss_thumbnails/vaccinesautosaved-200817134646-thumbnail.jpg?width=640&height=640&fit=bounds)
















































































