Download as PDF, PPTX
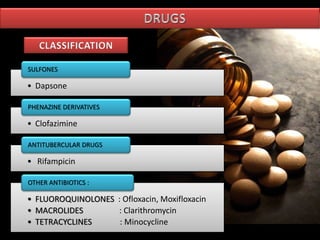
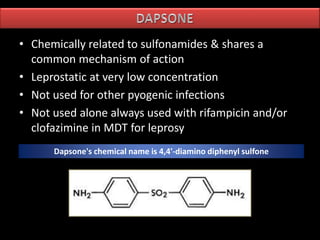
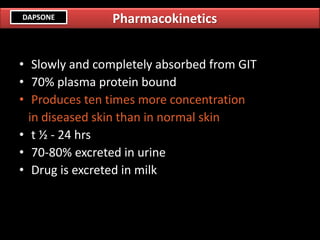
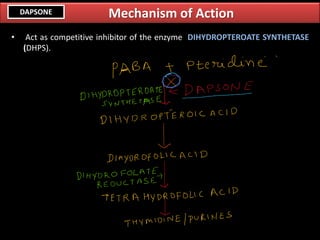



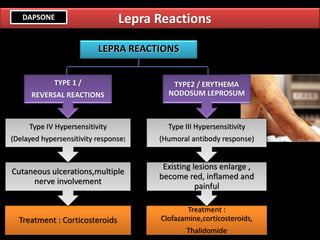
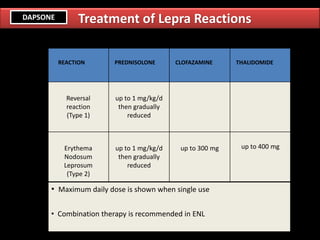

The document outlines the classification, mechanisms of action, pharmacokinetics, adverse effects, and treatment strategies for anti-leprosy drugs, including dapsone, clofazimine, rifampicin, fluoroquinolones, and macrolides. It details the treatment for different types of leprosy and lepra reactions, emphasizing multidrug therapy (MDT) and alternative regimens. The document also discusses the management of adverse effects and the implications of drug resistance.




































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)





![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)












