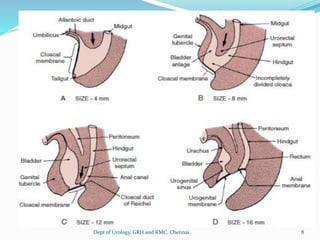
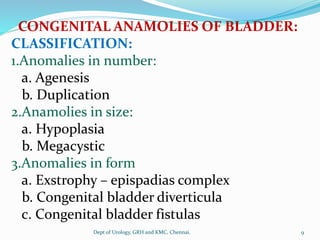
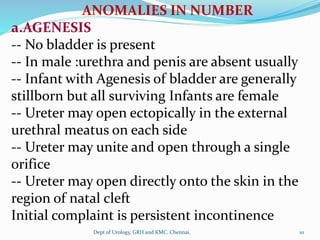
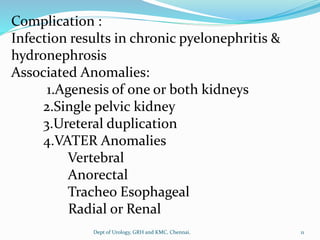
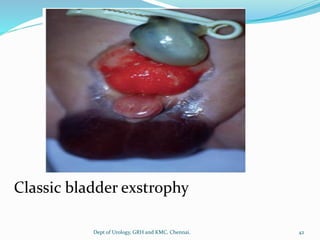
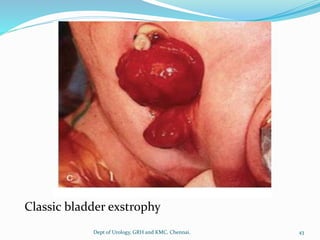
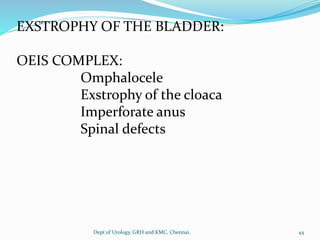
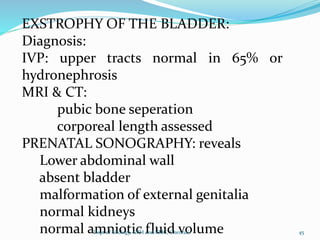
The document describes the embryological development of the urinary tract and various congenital anomalies that can occur. It discusses the formation of the urogenital sinus, cloaca, trigone, and bladder. It then categorizes and describes anomalies in number (agenesis, duplication), size (hypoplasia, megacystis), and form (exstrophy epispadias complex, diverticula, fistulas). Specific anomalies like complete duplication, sagittal septum, and classic bladder exstrophy are explained in detail.