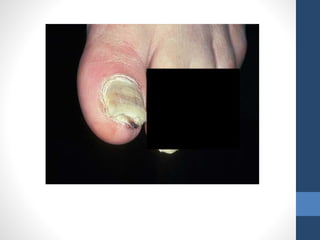
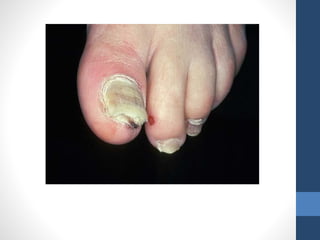
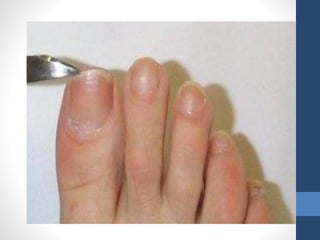
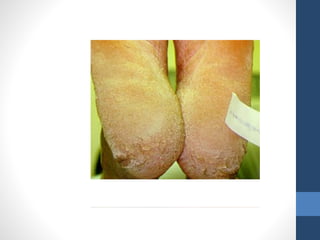
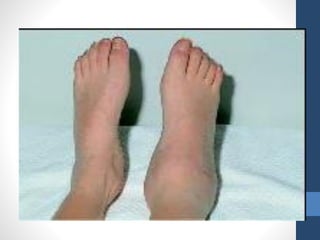
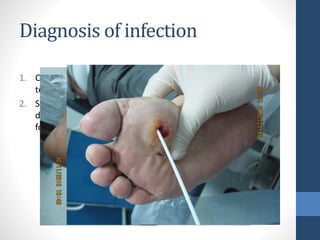
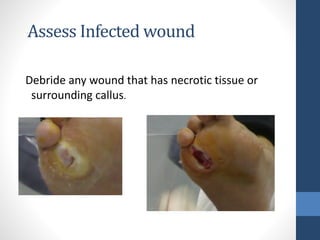
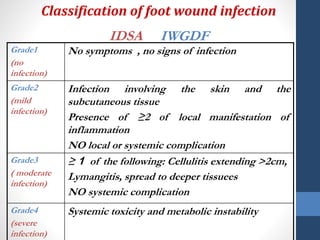
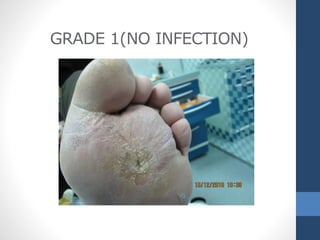
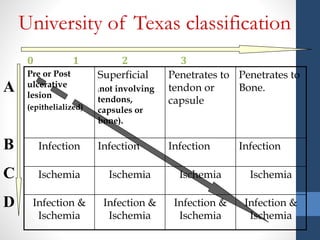
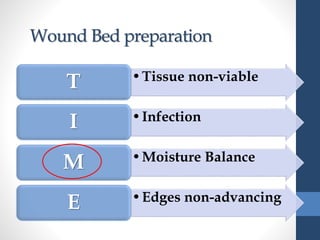
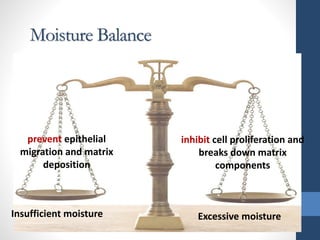
This document discusses some pitfalls in the treatment of diabetic foot ulcers. It begins by stating that no lesion should be underestimated. It then covers diabetic foot infection, describing the differences between contamination, colonization, and infection. Grading of foot wound infection from mild to severe is explained using the IDSA IWGDF classification system. The importance of debriding wounds with necrotic tissue is highlighted. Different dressings are discussed, noting that keeping wounds dry is no longer the preferred treatment and that some older antiseptics like Mercurochrome are no longer recommended. The concept of wound bed preparation focusing on issues of non-viable tissue, infection, moisture balance, and non-advancing edges is introduced











































































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)




