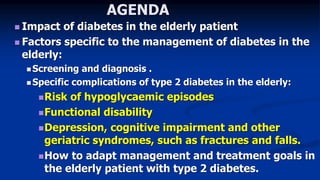
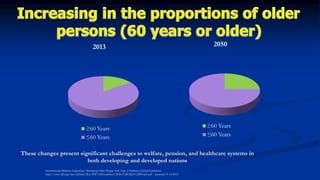
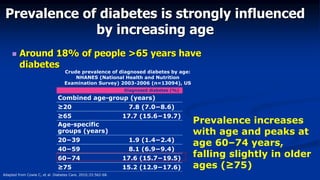
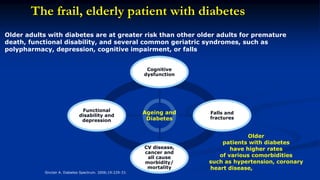
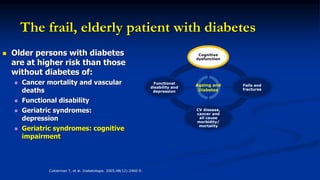
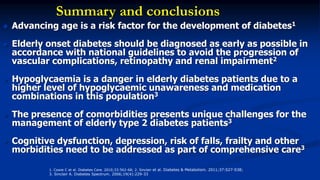
This document discusses diabetes management challenges in elderly patients. It notes that the prevalence of diabetes increases with age and peaks between 60-74 years of age. Screening and diagnosing diabetes in elderly patients can be difficult due to non-specific symptoms. Management goals aim to avoid hypoglycemia and other adverse drug reactions while controlling hyperglycemia and risk factors. The risk of hypoglycemia, functional decline, depression and other geriatric issues increases with age, requiring special consideration in diabetes management for frail elderly patients.




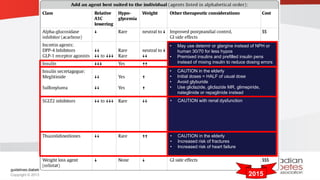
![In the frail elderly, while avoiding symptomatic
hyperglycemia, glycemic targets should be an A1C of
≤8.5% and FPG or pre-prandial PG of
5.0-12.0 mmol/L, depending on the level of frailty.
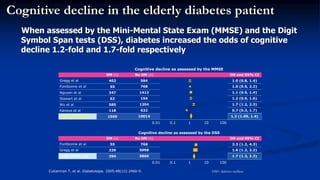
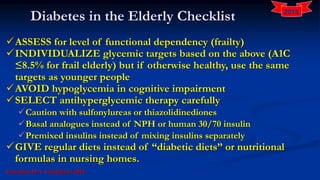
In elderly people with cognitive impairment, strategies
should be employed to strictly avoid hypoglycemia,
which include the choice of antihyperglycemic
therapy and less stringent A1C target [Grade D, Consensus].
Elderly people with type 2 diabetes should perform
aerobic exercise and/or resistance training, if not
contraindicated, to improve glycemic control [Grade B,](https://image.slidesharecdn.com/ueda2016-workshop-diabetesintheelderly-mesbahkamel-160404224107/85/Ueda2016-workshop-diabetes-in-the-elderly-mesbah-kamel-46-320.jpg)



























































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)















